 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
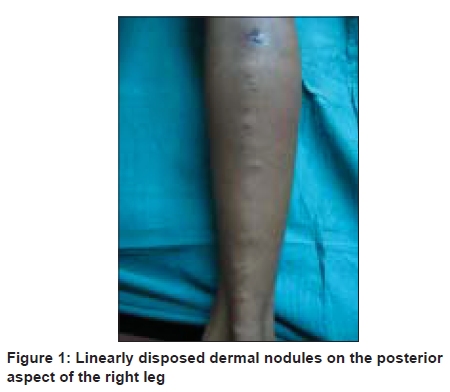
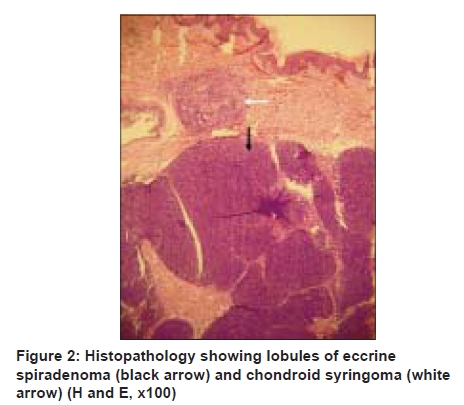
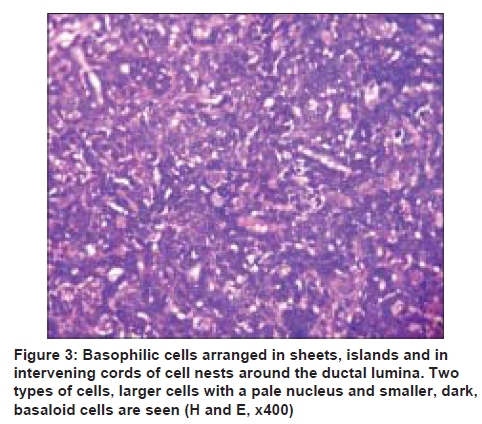
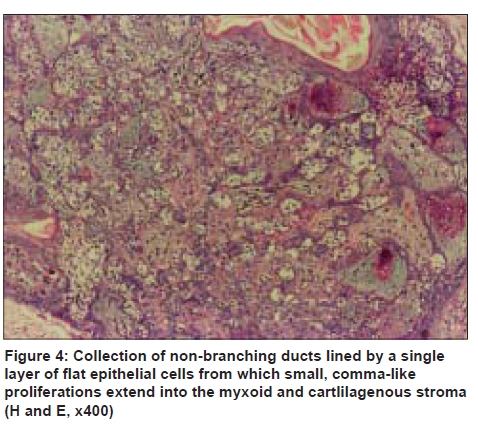
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 600-602 Case Report Eccrine spiradenoma with chondroid syringoma in Blaschkoid distribution Amiya Kumar Nath, Rashmi Kumari, Devinder Mohan Thappa Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 India Code Number: dv09204 PMID: 19915242 DOI: 10.4103/0378-6323.57723 Abstract Eccrine spiradenoma (ES) very rarely presents in a linear or zosteriform distribution. It may be associated with foci of various other appendageal tumors. We report a 14-year-old boy who presented to us with multiple nodules in a linear distribution in the posterior aspect of the right lower limb since 2 years of age. The lesions became significantly painful for the past 2 years. Histopathology revealed dermal lobules of ES with smaller foci of chondroid syringoma.Keywords: Blaschkoid, Chondroid syringoma, Eccrine spiradenoma, Linear Introduction Eccrine spiradenoma (ES) is an uncommon tumor of eccrine sweat gland origin, occurring mostly in young adults. [1] Incidence of ES is almost equal in both genders. [2] Most lesions occur as solitary, blue-red, dermal nodules on the upper, dorsal aspect of the body with a characteristic spontaneous pain or tenderness. [2] Multiple ES in a linear or zosteriform distribution is extremely rare. [3] Hereby, we describe a patient with multiple ES in a blaschkoid distribution with hitherto unreported coexistence of chondroid syringoma. Case Report A 14-year-old boy presented with multiple, raised lesions arranged in a linear pattern on the posterior aspect of the entire length of the right lower limb since 2 years of age. These lesions became prominent and significantly painful for the last 2 years. The pain was intermittent, dull-aching in nature and spontaneous in onset. On examination, multiple, small (0.5-1 cm), tender, bluish-to-reddish soft nodules were seen arranged in a linear pattern along the posterior aspect of the right lower limb extending from the buttock down to the ankle [Figure - 1]. These nodules became more prominent on standing. Ultrasound showed that the tumors were in the dermis. In Doppler ultrasound, vessels of the lower limb were found to be normal and the tumors showed no connection with the underlying vessels. Histopathology showed two well-discernible areas in low-power view. The predominant component was that of a well-circumscribed, multilobular dermal nodule consisting of aggregates of basophilic cells [[Figure - 2], black arrow]. On higher magnification, the basophilic cells were arranged in sheets, islands and in intervening cords of cell nests around ductal lumina. Two types of cells were seen - a more frequent larger cell with a pale nucleus in the center and smaller, dark, basaloid cells with hyperchromatic nuclei in the periphery [Figure - 3]. This picture was typical of ES. The smaller foci [[Figure - 2], white arrow] around the nodule of ES showed collections of non-branching ducts lined by a single layer of flat epithelial cells from which small, comma-like proliferations were seen to extend into a myxoid and cartlilagenous stroma [Figure - 4]. This was diagnostic of chondroid syringoma. A final diagnosis of ES with coexistent chondroid syringoma was made and surgical excision of the nodules in multiple sittings was advised. Discussion ES arises from the transitional area between the secretory portion and coiled duct of the eccrine apparatus. [3] The tumor is seen as blue-red dermal or subcutaneous nodules hence called "blue balls in the dermis." ES usually affects individuals in their second, third or fourth decade of life with predominant occurrence in young adults. It is uncommon in childhood, but no age is exempt. Lesions are often painless and non-tender. [3] However, spontaneous pain or tenderness on palpation is believed to be a characteristic symptom of ES. [2] The exact explanation for the pain in ES is not clear. It is said to be due to the contraction of myoepithelial cells, but electron microscopy has not proved the presence of myoepithelial cells in the tumor. [4] In histopathology, ESs have well-defined, multilobulated dermal and subcutaneous tumors comprising of two types of epithelial cells arranged in cords and sheets with evidence of ductal differentiation. [2] The larger cells with large pale nuclei are arranged in the center and smaller cells with hyperchromatic nuclei and scanty cytoplasm are arranged in the periphery. [2],[3] Perivascular spaces around the central blood vessels surrounded at the periphery by palisading tumor cells is as an important histopathological clue for diagnosis. [1] More than 97% of these lesions are solitary. [2] Multiple lesions may be seen in 2% of cases. [3] In our case, multiple nodules of ES were arranged in a linear configuration along the lines of Blaschko in the lower limb. Nevoid, zosteriform and linear arrangement of ES lesions along the lines of Blaschko are extremely rare. [2],[3] In such cases, the tumors have been proposed to arise from an organic hamartomatous process because of their frequent association with various appendageal components. [3] Rare features of ES include coexistence of cylindroma (or focal cylindromatous change), [2] eccrine hidradenoma, [1] trichoepithelioma [3] and pilar components. [1] Association of dermal cylindromas with spiradenomas may be due to identical stimulus for growth of these two types of tumors. [1] In our case, ES was associated with coexistent foci of chondroid syringoma. Familial (probably autosomal-dominant transmission) cases have also been described. [3] Sometimes, the lesions become highly vascular and attain a very large size, [1] up to 5 cm in diameter (giant ES). [2] Malignant transformation of ES (malignant spiradenoma or spiradenocarcinoma) has been described very rarely, presenting as a rapidly enlarging nodule within a long standing lesion. [2] Histologically, a clear transition zone between the benign and the malignant area can be detected in many cases. [5] Diagnostic features of a malignant transformation include markedly atypical cells with frequent mitoses, necrosis, loss of dual cell population and the loss of the lobular pattern that is normally characteristic for a benign spiradenoma. [5] No evidence of a malignant transformation was noted in our case. Surgical excision has been undertaken for isolated lesions of ES, but it may not be feasible for extensive lesions. [2] Other modalities of treatment like radiotherapy and CO 2 laser have been described in the treatment of CS in isolated reports, but their efficacy is not established. There is no satisfactory treatment for the pain. Chondroid syringoma is a rare, benign mixed tumor of the skin that arises from the sweat glands and contains a mixture of epithelial and mesenchymal tissues. [6] The term ''chondroid syringoma'' was coined because of the presence of sweat gland features in a cartilage-like stroma. [7] It is similar to pleomorphic adenoma arising from the salivary glands. [8] Headington classified condroid syringomas as apocrine and eccrine types based on their histopathological appearance. [7] This tumor is histopathologically identified by the presence of tubuloalveolar and gland-like structures with two or more cuboidal cell lines, islands of cuboidal or polygonal cells in a fibroadipoid, chondroid, hyaline or mucinous hypocellular stroma that positively stains for periodic acid-Schiff and Alcian blue. The eccrine type presents with smaller lumens lined by a single row of cuboidal epithelial cells and the apocrine type with tubular and cystic branching lumina lined by two rows of epithelial cells. Our case highlights a unique coexistence of ES and chondroid syringoma, presenting as multiple, painful, dermal nodules in a blaschkoid distribution. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09204f3.jpg] [dv09204f2.jpg] [dv09204f4.jpg] [dv09204f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}