 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 609-610 Images in Clinical Practice Norwegian scabies presenting as erythroderma Vandana Mehta, C. Balachandran, Puja Monga, Raghavendra Rao, Lakshmi Rao1 Department of Skin and STD, From the Dept of 1Pathology, Kasturba
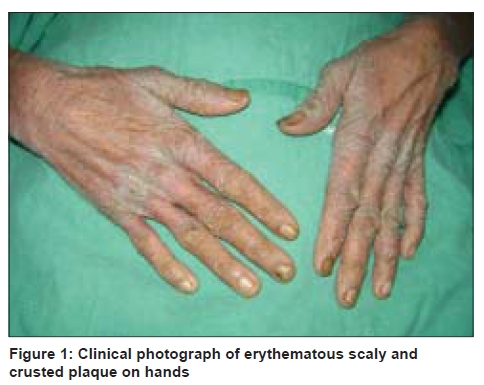
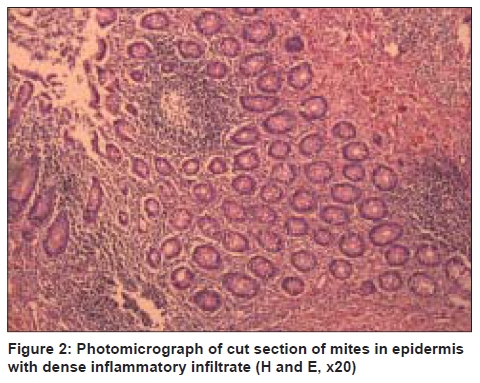
Hospital, Manipal - 576104, Karnataka, India Code Number: dv09207 PMID: 19915245 DOI: 10.4103/0378-6323.57726 A 70-year-old apparently healthy woman presented with generalized erythema and scaling of the body, of three months duration, for which she was on oral corticosteroids at the time of her presentation to us. She was a known asthmatic since many years. There was no past history of any preceding eczematous skin lesion. She reported intense pruritus which was severe during the nights. On further questioning she also revealed nocturnal pruritus and itchy lesions in several other family members. Cutaneous examination revealed generalized erythema and scaling with the presence of hyperkeratotic crusts accentuated on the palms, soles, cubital and popliteal fossae and scalp [Figure - 1]. A scraping for KOH mount from the crusted plaques on her hands, as well as a biopsy for histopathology revealed presence of numerous scabies mites, eggs and fecal pellets confirming the diagnosis of Norwegian scabies [Figure - 2]. Crusted scabies or Norwegian scabies (NS), as it was first described in lepers from Norway, is a clinically distinct and highly contagious form of scabies. In common scabies the number of parasites infesting the epidermis is relatively small. Such restriction is basically attributable to mechanical destruction of burrows by scratching; regular cleansing and cell mediated immune response. However, in NS, millions of mites colonize the epidermis inducing characteristic hyperplastic changes. NS results from a failure of the host immune response to control the proliferation of scabies mites in the skin, with resulting hyperinfestation and a concomitant inflammatory reaction. Patients chronically treated with immunosuppressive drugs i.e., post renal transplant patients, or those with HIV, HTLV I infection are more prone to develop NS. It has also been described in patients with severe systemic diseases such as (leprosy, rheumatoid arthritis, systemic lupus erythematosus) leukemia and in patients who do not scratch either because of an absence of pruritus or due to immobility such as in mental illness, sensory neuropathy, paresis and senility. Clinically, NS is characterized by extensive hyperkeratosis and crusting of the skin especially on the acral areas. A variable erythema is common evolving sometimes into erythroderma. The lesions are primarily distributed on the scalp, face, extremities, back and around the nail folds. Pruritus is usually absent or may be moderate to severe. In view of the hyperkeratosis and crusting diagnostic confusion with psoriasis, keratosis follicularis, contact dermatitis and seborrheic dermatitis may occur. A delay in diagnosis of even a single case of NS can lead to a massive outbreak of scabies among patients, health care personnel in hospitals and family members. Our patient was a healthy lady with no known risk factors for the development for NS, however, it could have been possible that simple classical scabies in her case was transformed to NS after the daily intake of corticosteroids which she had been consuming since the onset of her illness. Prolonged use of corticosteroids may induce NS, as was seen in our case. NS represents a serious therapeutic problem. It is very resistant to treatment, relapses frequently and in contrast to classical scabies where a single application of topical scabicidal would suffice, treatment application needs to be repeated every four to seven days. The introduction of oral ivermectin to therapeutic armamentarium has revolutionized the treatment of scabies. Our patient was treated with ivermectin 12mg which was subsequently repeated the following week along with topical scabicidal lotion (GBHC) with which her condition improved considerably. Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09207f1.jpg] [dv09207f2.jpg] |
| |||||||||

{kind=link}
{kind=link}