 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
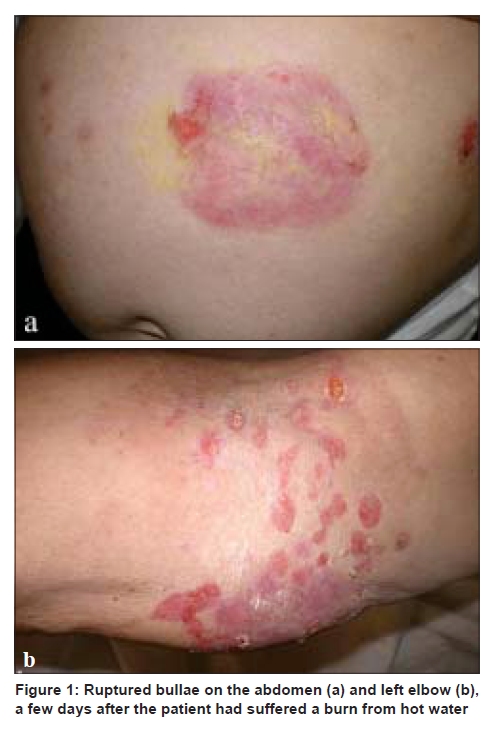
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 617-619 Letter to the Editor Trauma-induced bullous pemphigoid Chrysovalantis Korfitis, Stamatis Gregoriou, Sofia Georgala, Eleftheria Christofidou1, Iphigenia Danopoulou University of Athens, Department of Dermatology,
1Dermatopathology, A. Sygros Hospital, Athens, Greece Code Number: dv09213 PMID: 19915251 DOI: 10.4103/0378-6323.57732 Sir, Bullous pemphigoid (BP) is a common, autoimmune skin disease affecting the elderly. Furthermore, trauma has been uncommonly considered as a triggering factor for the disease. [1],[2],[3],[4],[5] We report two patients who developed BP associated with trauma. A 68-year-old housewife presented with numerous tense blisters on an erythematous base located on the trunk and limbs. A few days earlier she had suffered a burn from hot water on her abdomen and left arm resulting in the local formation of bullae, which she assumed to be due to the burn [Figure - 1]a-b. However, in the following days the bullous eruption became generalized involving areas that had not been previously damaged. The histopathology of a lesion showed subepidermal bulla with upper dermal infiltrate consisting of neutrophils and eosinophils [Figure - 2]. Direct immunofluorescence revealed the linear deposition of IgG and C3 at the dermoepidermal junction, whereas, the salt-split skin was consistent with BP. Treatment with prednisone 50 mg daily was initiated and BP remitted without recurrence. A 73-year-old man referred to our clinic exhibiting multiple intact bullae and erosions on his tegument and limbs. Two months earlier he had been submitted to a surgical procedure to treat his abdominal hernia. Subsequently, tense hemorrhagic bullae developed at the area of the postsurgical scar [Figure - 3] with the disease progressing to the trunk and limbs. No previous history of bullous eruption was reported. Skin biopsy and direct immunofluorescence were consistent with BP or epidermolysis bullosa acquisita. The patient was treated with prednisone 60 mg daily, with complete remission of the disease. Bullous pemphigoid presents with tense bullae either on erythematous or normal-appearing skin. Skin biopsy from a lesion revealed the existence of a subepidermal blister along with a dermal inflammatory infiltrate, primarily consisting of neutrophils and eosinophils. The diagnosis can be further supported by performing direct or indirect immunofluorescence showing IgG and / or C3 deposition along the basement-membrane zone or circulating IgG autoantibody, respectively. In order to exclude epidermolysis bullosa acquisita one should perform the salt-split skin technique or even electron microscopic examination. The Koebner or isomorphic phenomenon is the development of novel skin lesions at the sites of trauma in patients suffering from pre-existing dermatoses and it is best documented in psoriasis. [1] There have been rare reports incriminating trauma as the triggering factor for the induction of BP. However, the development of BP in these patients is considered as a poor or questionable trauma-induced process rather than a "true" Koebner phenomenon [1],[2] due to its infrequent exhibition and the lack of experimental evidence. Nevertheless, a number of cases have been published linking BP to various types of trauma such as burns, surgical wounds, [1] photochemotherapy, [3] radiation therapy, [4] and central venous lines or fistulas. [5] In our two patients, BP arose primarily in the traumatized skin, showing direct association with the trauma and only then it expanded to other areas of the body. As none of our patients had suffered previously from BP this association cannot be called a Koebner phenomenon by definition. Despite the fact that trauma-induced BP is an uncommon condition the clinician should be aware of this possibility and consider the diagnosis of BP in cases of appearance of blisters arising from wounds. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09213f1.jpg] [dv09213f3.jpg] [dv09213f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}