 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 620-622 Letter to the Editor An unusual case of dermatitis herpetiformis presenting with initial scalp localization Ülker Gül, Seçil Soylu, Aylin Okcu Heper1 Second Dermatology Clinic, Ankara Numune Education and
Research Hospital, Ankara, 1Department of Pathology, Ankara
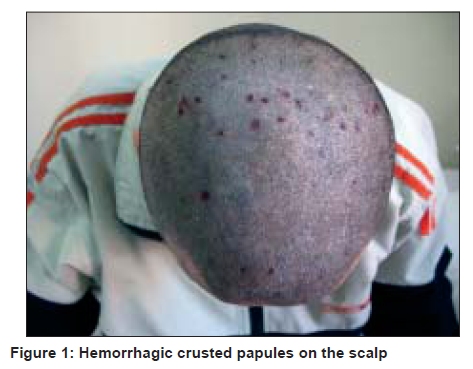
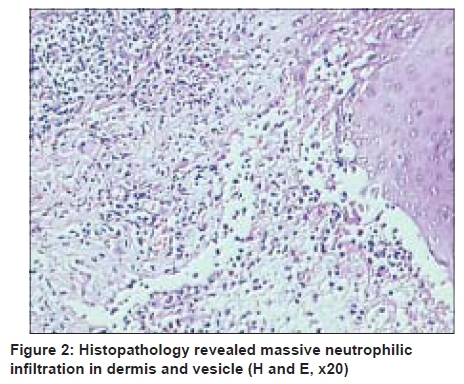
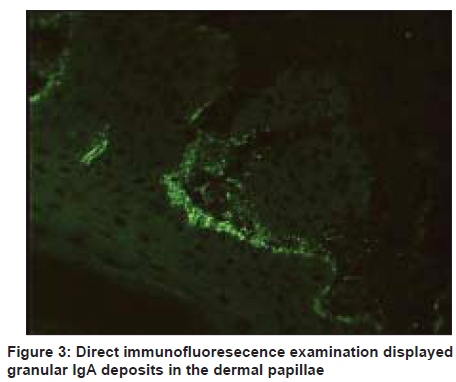
University, School of Medicine, Ankara, Turkey Code Number: dv09215 PMID: 19915253 DOI: 10.4103/0378-6323.57734 Sir, Dermatitis herpetiformis (DH) is a serious pruritic bullous skin disease that predominantly affects the extensor surfaces of the elbows, knees, buttocks, back, and scalp. [1],[2],[3] Although the scalp is a predilection site of DH, it is not a familiar localization site of onset of the disease. Here, in this report, a DH with onset only on the scalp is reported. In July 2007, a 30-year-old man developed itchy hemorrhagic crusted papules on the scalp without any lesions on the other parts of his skin [Figure - 1]. The patient stated that this rash had appeared three years ago, and he had consulted a physician, received topical corticosteroids and emollients with the probable diagnosis of eczema or folliculitis, which frequently recurred. He had no complaints of diarrhea, bloating, or abdominal pain. Physical examination revealed no abnormality. On histopathological examination of the lesions located on the scalp, subepidermal blistering with massive neutrophilic infiltration in the dermal papillae was revealed [Figure - 2]. Direct immunofluorescence examination displayed granular immunoglobulin (Ig) A deposits in the dermal papillae [Figure - 3]. On blood and serum analysis, iron deficiency anemia and folate and vitamin B12 deficiency were detected. Antigliadin IgA, IgG, and antiendomysium antibodies were negative. The chest radiography and ultrasonography of the abdomen were normal. The patient was referred to the hematology and gastroentereology clinics for evaluation of anemia and for a possible associated gastrointestinal abnormality, which could be due to gluten sensitivity. A fecal occult blood test was negative. Endoscopy revealed bulbitis and gastritis. In the examination of the pathological specimens, a partial villous atrophy was revealed. During the follow up period, multiple itchy - either excoriated or vesicular - hemorrhagic crusted erythematous papules and plaques were found on the face, back of both shoulders, elbows, and in the region of the glutea. The skin biopsy that was performed from these areas reconfirmed the diagnosis of DH. The patient was started on dapsone, iron-folic acid supplementation therapies and was recommended to follow a gluten-free diet. He is still on follow-up without any lesions. Dermatitis herpetiformis affects men more frequently than women, between the second and the fourth decades of life. [2] The hallmarks of the disease are the grouping of the lesions, their symmetry, and their distribution. [2],[4] However, the patient often presents with only multiple erosions secondary to scratching, as an intense itching is very characteristic of the eruption. The usual symmetric distribution of these lesions is on extensor surfaces, especially the elbows, knees, shoulders, sacrum, buttocks, and the posterior nuchal area. In some cases, the lesions may also involve the scalp, face, and groin. [1],[2],[3] However, until date, no data regarding the onset of DH on the scalp, except the case that is presented in this report could be observed in the literature. The diagnosis of DH is made by the classic skin presentations, but confirmation requires careful immunofluorescence staining, particularly of the perilesional biopsy specimens. In direct immunofluorescence examinations, granular IgA deposition at the dermoepidermal junction with stippling in the dermal papillae is pathognomonic of the condition. Patients who have DH present with partial villous atrophy in the biopsies of small bowel and a degree of damage in the intestine. [2] Endomysium antibodies and tissue transglutaminase antibodies are both serologic markers for gluten sensitive enteropathy in DH patients. [2],[5] Our case had a partial villous atrophy in the biopsies of the small bowel. In the differential diagnosis of DH localized to the scalp, pruritic scalp disorders such as erosive pustular dermatosis of the scalp and, lichen planopilaris, should be considered. Nevertheless, these diseases cause cicatricial alopecias clinically and immunofluorescence stainings are negative. [6] Linear IgA dermatosis often closely mimics the clinical pattern of patients with DH. The direct immunofluorescence of the perilesional skin of patients of linear IgA dermatosis, which discloses a homogenous band of IgA at the dermal-epidermal junction, discerns the disease from DH. [3] Suppressive therapy, with sulfones, predominantly dapsone and occasionally sulfamethoxypyridazine and sulfapyridine, rapidly suppress the skin reaction and are quite effective for DH. As the underlying cause of DH relates to the oral intake of particular proteins derived from wheat, barley, rye, and possibly oats, DH patients should be treated with a gluten-free diet therapy. [2] There are also studies that suggest the protective role of a gluten-free diet against gastrointestinal lymphomas, which were reported to be increased in patients with DH, in the literature. [3] However, DH is a well-known skin disease, and the scalp is a commonly involved site but the onset of DH on the scalp is very rare. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09215f1.jpg] [dv09215f3.jpg] [dv09215f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}