 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
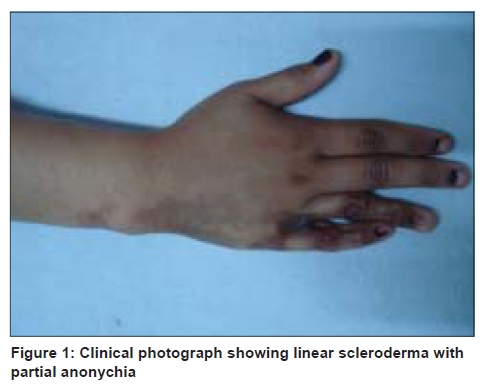
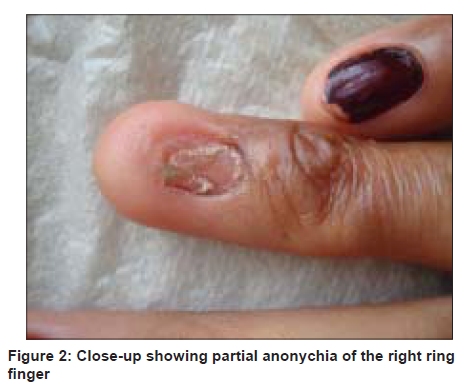
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 623-625 Letter to the Editor Linear scleroderma with partial anonychia Sanjay Singh, Surendra Kumar Department of Dermatology, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, India Code Number: dv09217 PMID: 19915255 DOI: 10.4103/0378-6323.57736 Sir, Linear scleroderma, a variant of morphea, is characterized by band-like induration of the skin, often with pigmentary changes, and it frequently occurs in children in the first or second decade. [1] The limbs are most commonly affected followed by the face. Various studies have shown different rates of frequency of different morphologic variants of morphea. A study of 239 patients with morphea, of which 126 were children, showed that 22 (17.5%) of the children had linear scleroderma. [2] Thus, although linear scleroderma is not a rare disease, yet, so far, no case of this condition with anonychia has been reported. We herein report a case of linear scleroderma with partial anonychia. A 22-year-old Indian girl presented with hyperpigmented linear macular and thickened lesions extending from the ulnar side of the middle of the right forearm up to the ring and little fingers for the past 10 years. The lesion first appeared on the middle part of the ulnar side of the right forearm and gradually progressed to involve the dorsal aspect of the little and ring fingers within 5 years. This included involvement of the nail of the ring finger, which led to partial loss of nail plate. The disease process has remained localized and static for the last 5 years. There was no history suggestive of Raynaud's phenomenon and there were no systemic complaints. Examination showed a brown-colored linear band-like lesion with irregular and sharp borders. The lesion was atrophic in the proximal part and demonstrated induration and binding down in the distal part [Figure - 1]. Hair was absent on the affected parts. The lesion was encroaching on the nail apparatus of the ring finger where partial anonychia with a small remnant of nail plate and loss of cuticle were present [Figure - 2]. There was ulnar deviation of the right ring finger and mild radial deviation of the little finger. Systemic examination was normal. Biopsy was taken from the proximal part of the lesion on the hand. Histopathology showed a sparse superficial and deep perivascular and periappendageal lymphohistiocytic infiltrate with occasional plasma cells [Figure - 3]. There was marked thickening of collagen bundles in the reticular and papillary dermis. The thickened bundles were generally parallel to the epidermis and were closely packed to give a hyalinized appearance. These findings were consistent with the diagnosis of scleroderma. As the lesion of scleroderma visibly involved the nail apparatus and biopsy from the lesion showed typical features of scleroderma [Figure - 3], we did not take nail matrix biopsy. Patient's urinalysis (routine and microscopy) was normal. Her rheumatoid factor was negative and antinuclear antibody (ANA) test revealed equivocal result. Some patients with linear scleroderma may be at some risk for developing systemic collagen-vascular diseases. [3] The present patient is being followed-up closely due to her equivocal ANA result. Among different variants of morphea, there is only one report of anonychia in a patient with pansclerotic morphea of childhood. [4] The same patient appears to have been reported again as part of a case series [5] because several details (age, weight, laboratory investigations, treatment and outcome) of these two cases match. No patient with linear scleroderma has been reported so far with anonychia. Basically, the loss of nail plate results from the involvement of the nail apparatus due to the sclerotic process. This change will be irreversible. Anonychia is generally described in textbooks as a congenital anomaly; acquired causes are usually trauma and lichen planus. [6] The present case shows, for the first time, that linear scleroderma can cause anonychia thus documenting a so far unreported cause of acquired anonychia. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09217f1.jpg] [dv09217f3.jpg] [dv09217f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}