 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 625-627 Letter to the Editor Tzanck smear finding of Dorfman-Chanarin syndrome Murat Durdu, Fahrettin Akay1, Tevfik Alper2, Serkan Yasar Çelik3 Baskent University Faculty of Medicine, Department of Dermatology,
Adana Hospital, Adana/Turkey, Department of 1Ophthalmology,
2Internal Medicine, 3Pathology, Diyarbakõr Military Hospital,
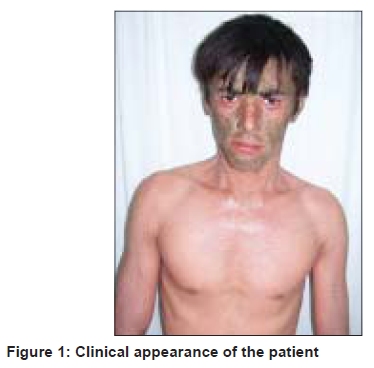
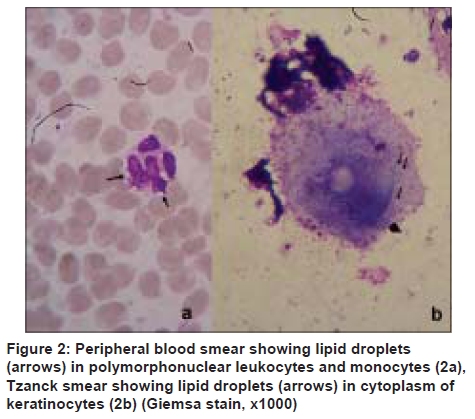
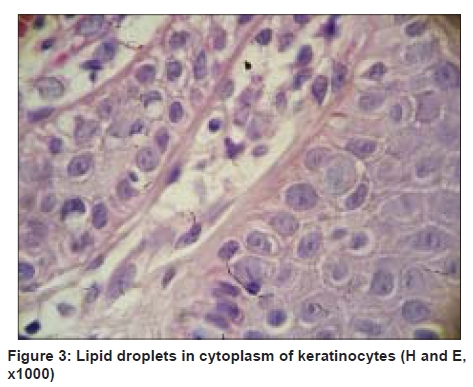
Diyarbakõr, Turkey Code Number: dv09218 PMID: 19915256 DOI: 10.4103/0378-6323.57737 Sir, Dorfman-Chanarin syndrome (DCS), also referred as neutral lipid storage disease with ichthyosis, is an autosomal recessive inherited disorder characterized by lipid vacuoles in peripheral leukocytes and several tissues. Genetic studies have identified a causative mutation in hydrolase CGI-58 gene on human chromosome 3p21. Because of these mutations, triacylglycerols accumulate in cytosolic droplets in multiple organs. [1] Tzanck smear findings of DCS were not reported previously. A 21-year-old man was admitted in the dermatology department with generalized ichthyosis present since birth. He had no family history of a similar condition. Dermatologic examination revealed generalized scaly skin lesions in face, abdomen, arms, and legs [Figure - 1]. There was marked involvement of flexures. The individual scales over the trunk were white, fine, translucent, and semiadherent while those on the face were grey brown scale-crust. Bullous lesions, erosions, and keratosis pilaris were absent. The palms, soles, teeth, and nails were normal. Ophthalmological examination revealed early corticonuclear cataract, hyperopia, and ectropion. Audiological examination revealed bilateral sensory neural hearing loss. Abdominal and neurologic examinations were normal. Laboratory parameters revealed increased levels of aspartate aminotransaminase (75 U/L; normal range: 0-40), alanine aminotransaminase (81 U/L; normal range: 0-40), and creatine phosphokinase (785 U/L; normal range: 25-175). The complete blood count, fasting blood sugar, renal function tests, thyroid function tests, lipid levels, albumin, and bilirubin were within normal range. Hepatitis markers were negative. Giemsa stained peripheral blood smear of patient showed lipid vacuoles in neutrophils consistent with Jordan's anomaly [Figure - 2]a. Chest X-ray, electrocardiogram, electromyelography, cranial computerized tomography were normal. Abdominal ultrasonography revealed increased echotexture suggestive of grade II-III steatohepatitis. Liver biopsy was planned, but the patient did not allow. After cleaning with alcohol, the skin of the face was grasped between the thumb and forefinger of the left hand. A superficial incision was made with a blade (no. 15) and the tissue was scraped through the incision. The cellular materials were then spread as a thin layer onto two microscopic slides and the air-dried specimens were stained by Giemsa. Tzanck smear examination showed vacuoles in the cytoplasm of keratinocytes [Figure - 2]b. Histopathologic examination of skin biopsy confirmed lipid vacuoles in keratinocytes [Figure - 3]. Based on the clinical, laboratory, and histological findings, a diagnosis of DCS was made. He was started on emollients and responded only minimally. In DCS, skin, liver, muscle, eye, ear, neurologic leucocytes involvement are frequent. [2] Clinical manifestations of this syndrome are ichthyosis (100%), hepatosteatosis (63.6%), myopathy (60.6%), sensorineural hearing loss (30.3%), growth retardation (21.2%), mental retardation (24.2%), cataract (42%), ectropion, strabismus (12.1%), nystagmus (9.1%), myopia (9.1%), and neurological symptoms. Lipid vacuoles in the leucocytes (Jordan's anomaly) are important diagnostic criteria of this syndrome and can be identified in 100% of leucocytes. [3] In our patient, who had hepatosteatosis, sensorineural hearing loss, cataract, hyperopia, ectropion, Jordan's anomaly, and raised levels of serum muscle enzyme, hyperopia has not been previously reported. The most common cutaneous finding of DCS is congenital nonbullous ichthyosiform erythroderma. Ichthyosis is often present at birth. Collodion baby, nonspecific ichthyosiform dermatosis, sparing of the face, generalized scaly erythematous plaques, erythematous scaly migrating plaques, hyperkeratosis on the palms and soles, cicatricial or diffuse alopecia are other dermatological manifestations. Nail involvement is absent in most of the cases, but transverse leuconychia, yellow-black discoloration, dystrophic or thickened nails, pitting and onychoschizia can be seen occasionally. [3] Histopathologically, examination of skin biopsy demonstrates hyperkeratosis, focal parakeratosis, moderate acanthosis, elongation of the rete ridges, lipid droplets in keratinocytes, prominently in the epidermal basal layer and in appendageal epithelia.[1] Furthermore, electron microscopic examination reveals cytoplasmic lipid vacuoles in many dermal cells, such as fibroblasts, pericytes, mast cells, and epidermal Langerhans' cells. [4] Tzanck smear test is an inexpensive, useful, and rapid diagnostic tool for certain skin diseases. It has been used in the diagnosis of various erosive-vesiculobullous, nodular and tumoral skin lesions during the following six decades. But, practice of cytodiagnosis in dermatologic diseases has been limited to herpetic infections, pemphigus, and cutaneous leishmaniasis.[5] In this case report, we demonstrated vacuoles in keratinocytes by cytologic examination. There is no effective treatment of DCS, but a diet low in long-chain fatty acids is reported to decrease skin and liver manifestations. Retinoids are useful in the treatment of skin and muscle manifestations. [2] Tzanck smear may provide important information in a patient with suspected DCS. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09218f2.jpg] [dv09218f3.jpg] [dv09218f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}