 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
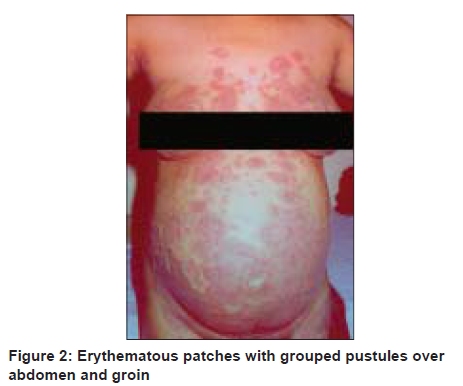
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 638 Net Case Generalized pustular psoriasis of pregnancy successfully treated with cyclosporine Debeeka Hazarika Department of Dematology, Assam Medical College and Hospital, Dibrugarh, Assam, India Code Number: dv09224 PMID: 19915261 DOI: 10.4103/0378-6323.57743 Abstract Two multigravidae aged 27 and 29 years, with previous uneventful pregnancies, second being psoriatic, reported at 24 and 28 weeks of pregnancies, with generalized pustular lesions. Laboratory findings, including serum calcium were normal. Ultrasonography showed normal fetal growth. Histopathology confirmed pustular psoriasis. Patients were put on cyclosporine 3 mg/ kg weight/ day after failure of an initial systemic steroid. Blood pressure, pulse, and fetal heart sounds were recorded every 12 hours, and ultrasonography and blood parameters, biweekly. Cyclosporine was tapered and stopped after delivery of two healthy babies at 38 weeks. We conclude that cyclosporine can be an option in the management of pustular psoriasis of pregnancy or psoriasis with pustulation in pregnancy.Keywords: Cyclosporine, Impetigo herpetiformis, Pustular psoriasis Introduction Impetigo herpetiformis is a rare pustular form of psoriasis, especially occurring in pregnancy with features of generalized pustular psoriasis, but with a tendency to be symmetrical and grouped, often starting in the flexures, and the constitutional disturbances may be severe. [1],[2],[3],[4] The onset is usually in the last trimester of pregnancy, but may be earlier and has been recorded in the first month of pregnancy. [2] The disease tends to persist until the child is born and occasionally even later. We report here two cases of pustular psoriasis in pregnancy, which were successfully treated with cyclosporine. Case Reports Case 1 A 27-year-old, 20 weeks pregnant female presented with pustular eruption on an erythematous background, over the neck, trunk, and flexures of the extremities, of one month duration. The skin lesions were associated with an intense itching and burning sensation. The patient gave a history of intermittent fever; the temperature rose up to 102 - 104°F during the evening hours. It was not associated with chills or rigors. The rise in temperature was also associated with a flare-up of the lesions. She did not give any personal or family history of psoriasis. Her earlier two pregnancies were uneventful. The patient did not give any history of other systemic illnesses. Dermatological examination revealed numerous minute pustules grouped together on acutely inflamed areas of the skin, coalescing to form bigger sheets of lesions, distributed over the neck [Figure - 1], upper part of the chest, abdomen, and back. Oral mucosa was normal. Examination of other systems revealed no abnormality. The patient was having a high temperature of 102 0 F at the time of examination. Obstetrical examination revealed 20 weeks of pregnancy with normal fetal heart sound. Laboratory investigations showed no significant changes of serum calcium level. Routine examination of blood, liver function tests (LFTs), and renal function tests (RFTs) were within normal limits. Gram stained smear examination of pustular eruptions revealed no bacteria and the pus culture was sterile. Baseline ultrasonography of the abdomen confirmed 20 weeks of gestation, with an active single fetus of normal growth. A histopathological study of the lesional skin revealed parakeratosis, elongation of rete ridges and dermal papillae, along with tortuous suprapapillary capillaries. Munro's microabscesses were evident at the lower end of the horny layer. The patient was put on 30 mg/day of prednisolone and regression of the lesions was observed within a week of therapy, and then the dose of steroid was tapered within three weeks time. As soon as the dose attained 10 mg /day, the lesions started reappearing, becoming extensive within a week with a high rise in temperature. The patient became very toxic and irritated. The patient was subsequently put on cyclosporine, at 24 weeks of pregnancy, on a dose of 150 mg/day (3 mg/kg body weight), in divided doses. The patient was monitored carefully for blood pressure, pulse, and temperature. The fetal heart sounds (FHS) were recorded at 12 hour intervals. During the therapy, investigations were conducted at an interval of two weeks and were found to be within normal limits. Ultrasonography of the abdomen was also done at the same interval, to monitor fetal growth. Fever, burning sensation, and erythema subsided on the next day of therapy. Skin lesions started regressing from the second day and complete resolution was noted after 10 days of cyclosporine therapy. The drug could not be withdrawn, as new lesions continued to appear, and she was maintained on 50 mg/day till 34 weeks of pregnancy. In spite of the maintenance dose, there was a flare-up of lesions and the dose was increased to 150 mg/day, up to the time of delivery. She gave birth to a healthy male baby at 38 weeks of pregnancy following lower segment cesarean section (LSCS). The treatment was stopped within three weeks of delivery after gradual tapering of the dose. The patient did not turn up for further checkup. Case 2 A 29-year-old female doctor, a known case of psoriasis for 15 years, presented at 28 weeks of gestation with multiple plaque-type lesions, studded with pustules, since two weeks. The lesions initially appeared on the medial side of the thighs and submammary region, and then gradually involved the lower abdomen and chest. The lesions were associated with burning sensation, pain, and low-grade fever. Her first pregnancy was normal. There was no family history of psoriasis. On examination, besides having erythematous, plaque-type lesions, she had pustular lesions; pockets of pus were hanging under submammary areas, abdomen, and perineum [Figure - 2]. Examination of the other systems showed no abnormality. The temperature was slightly raised. Laboratory investigations revealed a serum calcium level of 7 g/dl and an erythrocyte sedimentation rate (ESR) of 45 mm at the end of the first hour. Other biochemical findings were within normal limits. The pus culture was sterile and a gram-stained smear revealed no bacilli. Ultrasonography of the abdomen showed normal fetal growth. Diagnosis of psoriasis with pustulation was made on the basis of history and clinical findings. As the patient declined cyclosporine therapy, prednisolone 40 mg/day and calcium 1000 mg/day oral were administered. The patient did not show any improvement with steroid therapy, even after one week of therapy, and rather deteriorated, showing an appearance of widespread new lesions. Moreover, she developed severe gastritis. Prednisolone was then tapered and stopped within two weeks. Then she was put on cyclosporine 150 mg/day (3 mg/kg per weight) in two divided doses. The skin lesions started regressing dramatically from the second day onwards and complete resolution was obtained within 10 - 14 days. However, appearance of few new lesions continued till the thirty-seventh week of pregnancy. The drug was continued at 100 mg/day till delivery. She delivered a healthy female baby at the thirty-eighth week of pregnancy by LSCS. The dose of cyclosporine was gradually tapered and stopped after three weeks of delivery, subsequently in her first check up after one-and-a-half months she presented with a psoriatic plaque on her right leg. Discussion Pustular psoriasis of pregnancy is characterized by an acute eruption of erythematous patches studded with pustules at the margins, occurring usually in the last trimester of pregnancy and has been recorded in the first month of pregnancy. [2] The lesions originate at the flexures, then spread to the center and may become generalized; occasionally there may be painful oral erosions and involvement of subungual areas leading to onycholysis. The face, palms, and soles are commonly spared. The rashes may be pruritic or painful, accompanied by constitutional symptoms of fever, chills, malaise, diarrhea, nausea, and arthralgia. Rarely tetany, delirium, and convulsions occur, if the hypocalcemia is severe. The disease tends to persist until the child is born and occasionally long afterwards. [2] Recurrence has been described in up to nine pregnancies, and on subsequent use of oral contraceptive. [2],[3] Laboratory derangement includes leucocytosis, neutrophilia, elevated ESR, anemia, and hypoalbuminemia. Hypocalcemia has often been reported. [1],[2] Blood and pus cultures are negative. Differential diagnosis includes pemphigoid gestationis, pustular drug eruption, subcorneal pustular dermatosis, pemphigus vulgaris, and dermatitis herpetiformis. Pemphigoid gestationis usually occurs at the twenty-first week of pregnancy and may flare up immediately post partum, in contrast to impetigo herpetiformis. Moreover, the initial lesions consist of pruritic urticarial papules and plaques, target lesions, and annular wheals. Pustular drug eruption will have a definite drug-intake history. Subcorneal pustular dermatosis lesions also have flexural and trunk predilection, but the lesions are pustular from the beginning, flaccid, turbid, and often oval rather than circular. Some lesions show a level of pus with clear fluid above. Pemphigus vulgaris appears with tense vesicles or bullae, turning into flaccid blisters within a few days; oral involvement is frequent, and may precede skin lesions. Grouped itchy vesicular lesions, predominantly on the extensors, are a presentation of dermatitis herpetiformis, with asymptomatic oral mucosal involvement, without constitutional symptoms. In our patients, the onset of pustular eruption was at the midtrimester of pregnancy, in the flexures, with marginal pustules becoming generalized later. The rashes were accompanied with constitutional symptoms of fever, chills, malaise, and burning pain over the lesional skin. Laboratory findings revealed raised ESR and hypocalcemia in one patient, with pus cultures being negative. The unusual findings in our cases included the onset at the midtrimester without a history of recurrence. Pustular psoriasis of pregnancy is very rare and by 1982, only 200 cases have been documented. [2] The condition is serious. The more severe and longstanding the disease, the greater is the risk of placental insufficiency, leading to stillbirth, neonatal death, or fetal abnormalities. [3],[5],[6] Oral corticosteroid is the mainstay of treatment in the management of pustular psoriasis of pregnancy. Of late, cyclosporine as well as methotrexate have been used in this condition. [7],[8] Cyclosporine, which is categorized as pregnancy category 'C', has been successfully used at doses between 5 and 10 mg/kg weight daily, to treat cases that are refractory to a high dose of systemic corticosteroids. Cyclosporine is a natural cyclic peptide compound of 11 amino acids, metabolized in the liver by P450, 34A cytochrome, and excreted primarily by way of bile, through feces. Only 6% of the total dose is excreted in urine and minimally through breast milk. We advocated cyclosporine in two of our cases because of unresponsiveness and intolerability to oral corticosteroid. It was found to be effective, without any adverse effect to both mother and fetus. The drug was tapered and withdrawn a short period after delivery, to avoid possible side effects on the breast-fed baby. Moreover, spontaneous regression was also observed after delivery, which helped to withdraw the drug quickly. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09224f2.jpg] [dv09224f1.jpg] |
| |||||||||

{kind=link}
{kind=link}