 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 639 Net letter Congenital giant tufted angioma I. S. Reddy, S. V. N. Anuradha1, G. Swarnalata1 Departments of Dermatology, 1Pathology, Apollo Hospitals, Jubilee
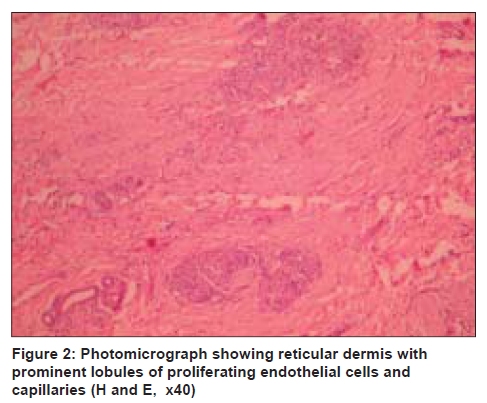
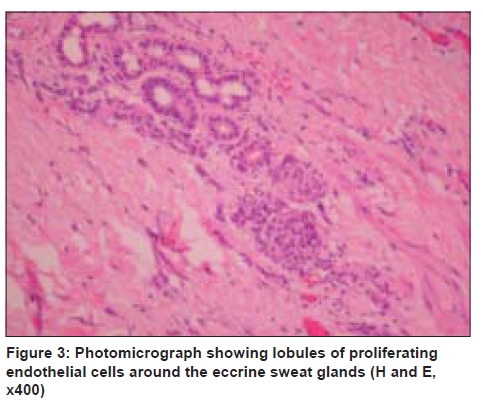
Hills, Hyderabad, India Code Number: dv09225 PMID: 19915265 DOI: 10.4103/0378-6323.57744 Sir, Tufted angioma is a rare, cutaneous, angiomatous proliferation described by Wilson-Jones and Orkin in 1989. The term "tufted angioma" was coined because of the characteristic dense clumps and lobules of endothelial cells and capillaries observed on histology. [1] Nakagawa in 1949 described the same condition as "angioblastoma" in Japanese children. Tufted angioma typically presents in the first few years of life as dull red or red brown patches and plaques of 2 cm to 5 cm over the neck, upper trunk, and proximal aspect of the limbs. Very few cases are reported with occurrence at birth, and lesions exceeding a size of 10 cm are a rarity. [2] A 30-year-old male presented with a well-demarcated, hyperpigmented, indurated plaque, 16 cm x 38 cm, involving the entire lower abdomen, extending from the umbilicus to the pubic area [Figure - 1]. It first presented as a bluish discoloration over the lower abdomen at birth and started increasing in its extent and insidiously became firm and indurated. Initially, the extension was toward the pubic area and upper thighs, which ceased after a few years. At the time of presentation, the spread was toward the umbilicus. The upper margin of the plaque showed a linear, tender, indurated, chord-like band. There was a well-defined, hemispherical, nontender, noncompressible, boggy swelling, abutting the lower margin of the plaque. A few satellite, hyperpigmented papules were present over the thighs in the periphery of the main lesion. The patient denied any history of bleeding or ulceration of the plaque. There was no evidence of sweating or excessive growth of lanugo hair over the plaque. Thrill and bruit were absent over the plaque. Hamartoma of connective tissue origin, morphoea, and Kaposi's sarcoma were considered as the clinical differential diagnoses. Skin biopsy was performed from the advancing margin of the plaque, just below the umbilicus. On histopathological examination, it showed multiple ovoid and round lobules of endothelial cells and capillaries arranged in a typical cannon ball distribution in the reticular dermis and subcutis [Figure - 2]. The capillary lumina were devoid of red blood cells. Proliferation of eccrine sweat glands adjacent to the vascular lobules was also observed [Figure - 3]. The stroma between the vascular lobules showed dense fibrosis correlating with sclerotic clinical presentation. Based on the characteristic histopathological features and clinical presentation, the diagnosis of congenital giant tufted angoima was made. The patient was advised to use clobetasol propionate cream over the tender and chord-like margin of the plaque and advised to review after four weeks, but was lost to follow up. Tufted angima is a rare, benign, and distinctive angiomatous condition, usually occurring between the ages of one and five years, and involving both sexes equally. Occasionally, the lesion can be present at birth, delayed onset in fifth and sixth decades have been reported. [1] It has been reported in a patient after liver transplant, but the lesions spontaneously resolved in two months, without any specific treatment. [2] It has been observed in pregnancy with resolution after delivery. [3] Familial cases have also been described. [4] As observed in our patient, tufted angioma showed a growth phase followed by a stabilization phase, and later, the lesion persisted indefinitely. The bright red color observed in capillary and cavernous hemangiomas is not seen in the tufted angioma, because of the deep location of the proliferating angiomatous elements and absence of red blood cells in the vascular channels. Apart from the usual morphology of papules and plaques, annular plaques with marked central depression have been reported. [5] Sweating over the plaque on exposure to heat or sunlight has been reported. [6] Growth of fine lanugo hair within the lesion has been observed. Platelet trapping and thrombocytopenic coagulopathy producing the Kasabach-Merrit phenomenon, is an uncommon complication of tufted angioma. [7] Histopathology shows scattered lobules or tufts composed of hypertrophied endothelial cells, pericytes, and capillary vessels in the reticular dermis, giving the characteristic cannon-ball appearance. Occasionally, the tufts coalesce to form irregular tracts of angiomatous tissue extending beyond the reticular dermis into the deep fascia and muscle. [8] An individual lobule is composed of cells with spindle and oval nuclei. Mitoses are extremely rare and there is no cellular atypia. Tufted angioma and Kaposiform hemangioendothelioma, sometimes show overlapping histopathological features. [9] In Kaposiform hemangioendothelioma, sheets of spindle cells show discrete aggregates of epithelioid endothelial cells and hyaline globules. Well-formed vascular channels showing intraluminal thrombi are often seen at the periphery of the tumor nodules. In difficult cases, immunohistochemistry for D 2 -40 may be helpful. Kaposiform hemangioendothelioma show positivity for this marker. Various treatment options are available for the tufted angioma. The recurrence rate is very high after surgical excision. Few cases have shown good response to a high dose of systemic steroids. [10] Subcutaneously administered interferon alpha has shown a significant response in a child with tufted angioma involving the jaw and neck. [8] An acquired tufted angioma over the left scapula with response to pulsed dye laser has been reported. [11] This case is presented for its congenital onset, which is rare, as also for the giant size of the skin lesion. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09225f2.jpg] [dv09225f3.jpg] [dv09225f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}