 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 6, November-December, 2009, pp. 639 Net Quiz Nodule on the chest Saurabh Agarwal, Binay Kumar1, Naveen Sharma2 Departments of Dermatology and Venereology, 1Pathology, 2Surgery,
Uttarakhand Forest Hospital Trust Medical College, Haldwani
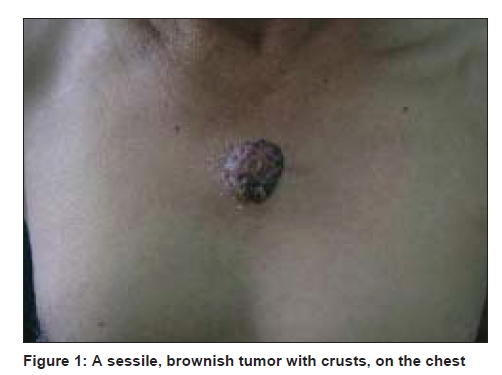
(Nainital) Uttarakhand - 263 169, India Code Number: dv09227 PMID: 19915263 DOI: 10.4103/0378-6323.57746 A 55-year-old male presented with an asymptomatic nodule on the chest for the last six years. It started as a pink-colored papule that gradually grew to the present size tumor, in two years. Subsequently the size of the tumor remained almost static. The tumor used to bleed a little, occasionally. There was no history of pruritus or pain in the tumor. No previous history of trauma to the area could be elicited. His medical and family history was noncontributory. Cutaneous examination revealed a 3.5 x 2.8 x 1.6 cm, well-circumscribed, brown-colored, sessile tumor on the sternum manubrium [Figure - 1]. The surface was rough with reddish-brown crusts and erosions at places. The tumor was firm, nontender, and did not bleed when touched. There was no regional lymphandenopathy. The histopathological findings are shown in [Figure - 2]. What is the Diagnosis ?
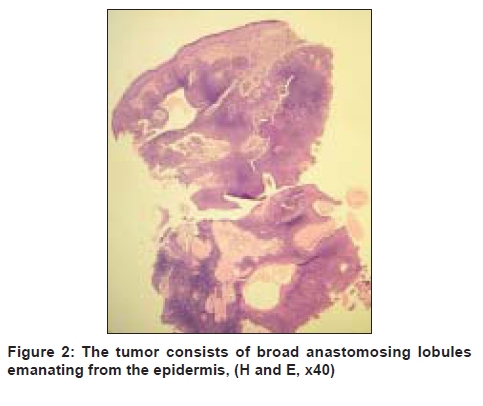
Histopathological findings The histopathology [Figure - 2] showed broad anastomosing tracts of cuboidal cells, with uniform nuclei originating from the epidermis. Tubular structures and cystic spaces were present within the neoplasm. The background stroma contained eosinophilic hyalinized collagen, and several large and small vessels were seen, especially under epidermis. Pigmentation was noted at the periphery of the tumor masses and occasionally within the masses. Pigment incontinence was also present. There was no horn cyst or palisading in the tumor masses. There was no atypia, mitosis, or necrosis. Discussion Eccrine poroma (EP), as first described by Goldman et al.[1] in 1956, is a benign tumor of the intra-epidermal portion of the eccrine sweat duct. These tumors typically present as solitary, sessile, or slightly pedunculated asymptomatic papules or nodules protruding from a cup-shaped depression. They are usually firm, fleshy lesions, pink-to-red in color, and may be lobulated. Eccrine poromas are usually seen in patients over 40 years of age, and have no predilection for a particular race and sex. The most common sites of involvement, as described by most textbooks, are the soles and palms. Hyman and Brownstein [2] reported 45 cases of EP and indicated that approximately 65% of EP erupted on the sole, 10% on the hand, and 25% on the hair-bearing areas of the body. In our case EP was present over the chest (sternum manubrium), an unusual site. To the best of our knowledge, there are a few reports of EP occurring on the chest. [3] The other unusual sites of involvement reported are, the scalp, neck, nose, eyelids, and pubic area. [3],[4],[5] The size of eccrine poroma usually varies from 0.2 to 1.5 cm and rarely exceeds 2.0 cm in diameter. [3] However, in our present case, it was quite large, measuring 3.5 cm in the largest diameter. The treatment of eccrine poroma is complete surgical excision, which was done in our case also. Malignant transformation (eccrine porocarcinoma) may occur in longstanding EP. [6] Sometimes, clinically, eccrine poroma may exhibit polymorphic features that can make the diagnosis difficult. Clinical differential diagnosis of eccrine poromas described in previous case reports includes pyogenic granuloma, hemangioma, seborrheic keratosis, verruca, fibroma, melanoma, nevus, cysts, and basal and squamous cell carcinoma. [3],[4],[5] Eccrine poroma is one of the variants of poroid neoplasms (PN), which are benign neoplasm accounting for 10% of sudoriferous tumors, or the so-called "sweat gland tumors". [3] The other PN are hidroacanthoma simplex, dermal duct tumor, and poroid hidroadenoma. Poroid neoplasms are composed of cells that are similar to those in the uppermost segment of the intradermal eccrine ducts and in the lower segment of the intraepidermal (acrosyringeal) eccrine ducts. Eccrine poroma arises within the lower portion of the epidermis and it proliferates downward into the dermis, consisting of broad anastomosing bands of epithelial cells. [7] The tumor cells are smaller than the epidermal keratinocytes, have a uniform cuboidal appearance, a round basophilic nucleus, and are connected by intercellular bridges, which are not always visible with a light microscope. The tumor cells contain a significant amount of glycogen. In most of the cases, narrow ductal lumina or cystic spaces may be found, as seen in our case also. Histopathologically eccrine poroma should be differentiated from basal cell carcinoma and seborrheic keratosis. In basal cell carcinoma, the cells have no visible intercellular bridges, are more variable in size, often show peripheral palisading, and contain little or no glycogen. Seborrheic keratosis has an even demarcation at their lower border; moreover, their cells have a potential to keratinize and form horn cysts. Microscopically, eccrine poroma usually lacks melanocytes and melanin pigmentation. However, coexistence with melanocytes in the tumor masses, in eccrine poroma, has rarely been reported. [3] Pigmentation, if present, is usually observed at the periphery of the tumor nests, as seen in our case also. The derivation of the melanocytes in the tumor nests of eccrine poroma is as yet uncertain. It is suggested that melanocytes in the tumor masses may migrate from the adjacent epidermis. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09227f2.jpg] [dv09227f1.jpg] |
| |||||||||

{kind=link}
{kind=link}