 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
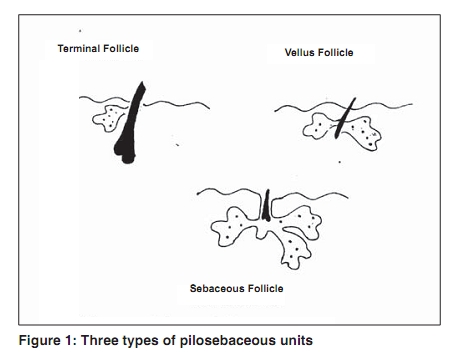
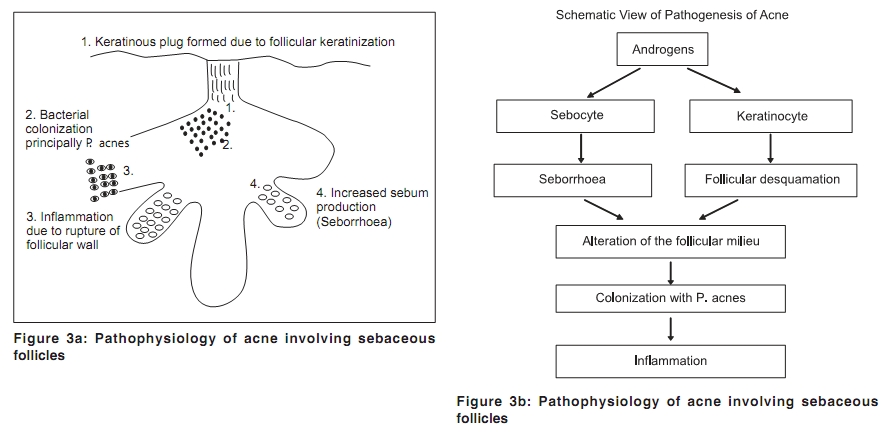
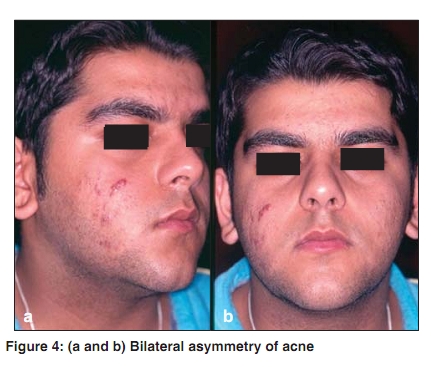
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 5-9 Acne in India: Guidelines for management - IAA Consensus Document Pathogenesis of acne Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09233 Acne represents obstruction and inflammation of the sebaceous follicles, a subtype of pilosebaceous units [Figure - 1]. [1] Sebaceous follicles show dominant sebaceous gland and rudimentary hair. The primary and pathognomonic lesion of acne is microcomedo, a microscopic lesion invisible to the eye. Some microcomedones evolve into either a noninflammatory comedo (open or closed), or an inflammatory lesion such as papule, pustule, or nodule [Figure - 2]. [2] The formation of a microcomedo requires a complex interplay of altered follicular keratinization, hyperplasia of sebaceous glands, and overcolonization of sebaceous follicles with Propionibacterium acnes [Figure - 3]. Host immune response and inflammation also contribute to clinical picture and course. [2] Altered follicular keratinization: The primary change in the sebaceous follicle is the alteration in the pattern of keratinization within the follicle. [3] Initial alteration is in the infrainfundibular portion where there is hyperproliferation. The excess keratin is also qualitatively altered as it tends to become densely packed along with monofilaments and lipid droplets. [2] Comedogenesis occurs when abnormally desquamated corneocytes accumulate in the sebaceous follicle and form a keratinous plug. [4] When the keratinous plug enlarges below a very small follicular pore at the skin surface, it becomes visible as a closed comedone (whitehead). An open comedone (blackhead) occurs if the follicular pore dilates. The small pore closed comedones are the precursors of inflammatory lesions. The closed comedones are the most frequent noninflamed clinical lesions and outnumber open comedones by a factor of four. [1] Subsequent proliferation of P. acnes generates inflammatory mediators and formation of inflammatory lesions. [5],[6] Immunohistochemical studies have shown an increase in the proliferation rate of the basal keratinocytes and abnormal differentiation of the follicular keratinocytes in the follicle wall of microcomedones and comedones.[4],[7],[8] These abnormalities may possibly be due to a relative decrease in sebaceous linoleic acid.[9] An androgen controlled defect may also contribute to abnormal proliferation through the 5-a reductase enzyme (type 1) in the infundibulum. [10] Follicular hyperproliferation is also associated with abnormal lipid inclusions (indicates abnormal differentiation).[6],[11],[12],[13] Cytokines are also involved in comedogenesis. High levels of biologically active interleukin-1α (IL-1α) have been detected in comedones, believed to be expressed by follicular keratinocytes and triggered by changes in sebum composition and secretion. [14],[15] IL-1α may compromise follicular barrier and thus induce inflammation. [15] Seborrhea and sebaceous gland hyperplasia: The sebaceous glands start to enlarge with androgenic stimulus at 7-8 years of age (adrenarche), with a net increase in sebum excretion. [16],[17] The overall size of the sebaceous follicles increases along with number of lobules per gland. [18] Acne subjects, male and female, excrete more sebum than normal subjects, [19] and the sebum excretion rate correlates well with severity of acne. [20],[21] Sebocytes and follicular keratinocytes are capable of metabolizing androgens through enzymes 5-a reductase (type 1), and 3b and 17b hydroxysteroid dehydrogenase. [10],[22],[23],[24],[25] These enzymes are present in undifferentiated basal sebocytes and with time the sebocytes differentiate and rupture releasing lipids into the sebaceous ducts. [26] The differentiation of the sebocyte is initiated by androgen uptake into the cell and its coupling with the cytoplasmic androgen receptor which, in turn, stimulates gene transcription and differentiation. [8],[22],[27] The increase in sebum production is mainly due to a difference in the response of the target organ (sebaceous follicle), to an increase in circulating androgens, or both. The target-organ responsiveness is variable and may be the explanation for the bilateral asymmetry of acne [Figure - 4] and [Figure - 5]. [28] In vitro studies have shown that sebocytes from different areas of the body have different responses to dihydrotestosterone and testosterone. [29] Sebocytes from the leg have a lower response or do not respond, whereas those from the face show a dose-dependent proliferation. [29] Bacterial colonization: P. acnes , an aerobic diphtheroid, is a normal skin resident and the principal component of the microbial flora of the pilosebaceous follicle. [30] In acne, the abnormal accumulation of corneocytes and the excess of sebum in the infrainfundibular portion of the duct is an ideal milieu for it to proliferate. [31] There is a correlation between colonization of the pilosebaceous duct and the onset of the microcomedo. There is no correlation between skin surface counts of P. acnes and the severity of acne [32] and yet it is also stated that P. acnes counts increase at each stage of acne as the follicle progresses from normal to comedone to an inflammatory lesion! [33] There is, however, correlation between the reduction of P. acnes and the clinical improvement in acne. [2] This reduction in P. acnes is associated with a reduction in proinflammatory mediators. [26],[34],[35] P. acnes is also being linked to toll-like receptors (TLR). TLR is a mammalian homologue of a drosophila protein known as toll that has emerged as a key regulator of host responses to infection. [36] Drosophila is a genus of small flies and includes many species of fruitflies. TLR is a transmembrane protein with a cytoplasmic portion homologous to IL-1 receptor. P. acnes bind to and activate TLR-2 which induces a cascade of signaling events involving monocytes and other inflammatory cells, and inflammatory cytokines. [37] The occurrence of such events has been confirmed in in vivo studies of inflammatory lesions in facial acne. [38] P. acnes also produce porphyrins which have become the target of novel light-based acne therapies. [39] The complete genome of P. acnes has been sequenced and has revealed a single circular chromosome of 2,560,265 base pairs, 2333 putative genes, and numerous gene products including sialidases, neuraminidases, endoglycoceramidases, lipases, and pore-forming factors. [40] Inflammation and immunological factors: Inflammation is the key component of acne and the major reason for its morbidity and sequelae (pigmentary disturbances and scarring). Inflammation, for a long time was believed to be a secondary process in the pathogenesis of acne. New data indicate that immunological events led by perifollicular helper T-cells in genetically predisposed individuals may in fact be a primary process, initiating comedogenesis through elaboration of IL-1. [41] Further, inflammation may upregulate sebum production through production of inflammatory mediator leukotriene B4 that binds to receptors on the sebocytes. [41] Sebum production is also influenced by neuropeptides - substance P and its degrading enzyme neutral endopeptidase - that may explain stress-induced aggravation of acne. [42] P. acnes may directly contribute to inflammation through generation of proinflammatory lipases, proteases, hyaluronidases, and chemotactic factors. [30] Lipases hydrolyze triglycerides to form free fatty acids which are comedogenic and primary irritants. At the cellular level, inflammation begins with an influx of CD4+ T-lymphocytes. Later, macrophages, Langerhans cells, and cells expressing HLA-DR are present. [42] There is also angiogenesis and vascular adhesion molecule expression. [43] The propensity for acne scarring varies between individual acne patients and is independent of disease severity. [41] A histopathologic study [43] has shown differences in the character of the cellular infiltrate and in the speed of evolution and resolution of inflammation. In sequential biopsies, it was observed that in patients who tended to scar, the immune response was milder initially and evolved slowly (compared to nonscarring patients), but it was more specific in cellular detail, and the inflammation persisted for a longer duration. [43] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09233f3.jpg] [dv09233f5.jpg] [dv09233f2.jpg] [dv09233f1.jpg] [dv09233f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}