 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
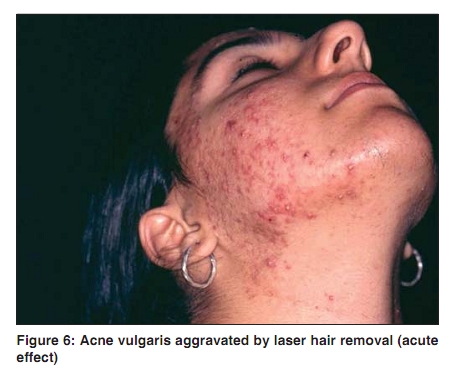
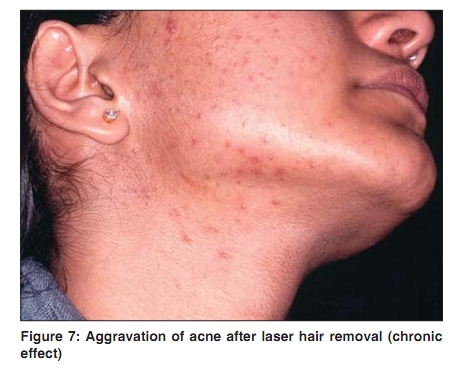
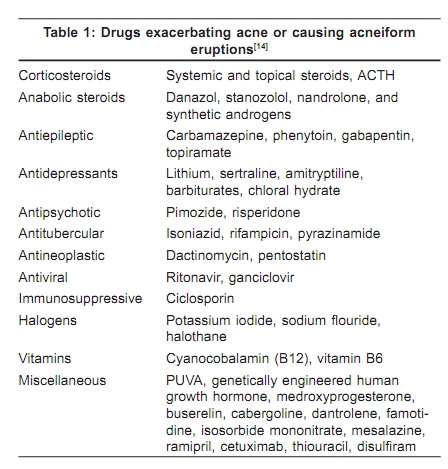
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 10-12 Acne in India: Guidelines for management - IAA Consensus Document Factors precipitating or aggravating acne Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09234 Acne is typically vacillating in its course. There are periodic flares, some of which may be accounted for by various triggers and aggravating factors. It is therapeutically rewarding to identify the concerned triggers and aggravating factors and be able to deal with them. Oils: In India, use of vegetable oils, coconut oil, almond oil, olive oil, and rye oil is popular. Such oils are traditionally used as moisturizers and revitalizers (as body rubs), and for hair dressing. Oils form an occlusive film over the applied area and cause comedogenesis and aggravation of acne in the acne-prone areas. Oils also cause folliculitis in the scalp, and on the limbs and torso. Oil folliculitis sometimes complicates pre-existent acne. In southern India, mineral-oil based pomades are popular and frequently cause acne on the forehead. Occupational exposure to industrial greases, oils, and petroleum products may cause folliculitis, and trigger acne. [1] Facials (facial massage): Facials are popular and are regularly undertaken by women in urban areas for a feeling of freshness, rejuvenation, suppleness of skin, tightening of skin, and for delaying the onset of wrinkles. [2] Facials were observed to have caused acneiform eruptions in 33.1% of subjects in a study in India. [2] These eruptions are characterized by deep nodules and closed comedones and show predilection for the cheeks. [2] Facials, therefore, are known to have the potential to aggravate acne. Cooking: While Indian food, rich in spices and oils, may not directly cause acne, the repeated exposure to oil vapors during cooking may do so, akin to McDonald′s acne. Cosmetics: Many cosmetics including some sunscreens are comedogenic (acne cosmetica/acne venenata). Some well-known comedogenic cosmetic ingredients are: isopropyl myristate, cocoa butter, lanolin, butyl stearate, stearyl alcohol, and oleic acid. Friction and pressure: Friction and pressure from helmets, backpacks, and tight collars can induce comedones and papules. Repeated irritation: Follicular irritation from shaving, waxing, threading, and laser hair removal [Figure 6] and [Figure 7] is sometimes associated with papules and pustules. Sweat: Sweating in a hot humid environment causes deterioration in 15% of acne patients. [3] Menstruation and acne: Premenstrual flare of acne reportedly occurs in 70% of female acne patients. [4] In a specially designed study, [3] lesional counts were performed during the follicular phase and late luteal phase over two cycles; in 63% of study patients, who were not receiving any treatment, there was on an average 25.3% increase in inflammatory lesions and 21.2% increase in comedones, from the follicular to the luteal phase. [5] Typically, the patient experiences a fresh breakout of inflammatory lesions, often 1-2 in number, on or near the chin, in the week preceding the commencement of the menstrual flow. The explanation offered is hydration-induced cyclical narrowing of the pilosebaceous orifice between days 16-20 of the menstrual cycle. [4] Progesterone and estrogen have pro- and anti-inflammatory effects, and alteration or modulation of these hormones may be another explanation. [4],[6] Pregnancy and acne: Pregnancy has an unpredictable effect on acne. Pre-existing acne may aggravate or remit during pregnancy. Stress: Stress is frequently implicated in aggravation of acne (vide supra) while acne itself induces stress. Sunlight: Sunlight is generally beneficial to acne although psoralens and UVA (PUVA) therapy may sometimes induce or aggravate acne. [7] There is also a report of Europeans developing a type of acne after a beach holiday (acne Mallorca). [4] A similar phenomenon has been observed in India and is locally referred to as ′Goa acne′. Smoking: There is no clear association between the two. One study showed a linear relationship between acne prevalence and the number of cigarettes smoked daily. [8] Another study suggested that severe acne was less common in smokers compared to nonsmokers. [9] A more recent cross-sectional study has concluded that the anti-inflammatory effects of smoking may inhibit the development of papulopustular acne, more so in girls than boys. [10] Diet and acne: Some recent literature has suggested links between acne and diet. A retrospective analysis of a large database in the USA, in which dietary intake of dairy products in high school students were correlated with physician diagnosed severe acne in women, a positive association was established.[11] It was hypothesized that milk and dairy products carry hormones and bioactive molecules that have the potential to aggravate acne. In another epidemiologic study, data were presented to suggest that high glycemic load foods (sugared foods) were the explanation for rising prevalence of acne in developed societies. [12] Hyperglycemic food intake results in increase in insulin like growth factor 1(IGF1) and a decrease in insulin like growth factor binding protein 3 (IGFBP3) leading to hyperandrogenism, seborrhea, and follicular hyperkeratosis. [12] However, the precise role of diet in the pathogenesis of acne remains unclear and controversial, and many dermatologists continue to propagate the conviction that acne is independent of diet. Drug-induced acne: This is well known. The best known causative drugs are halogenated compounds, progestogens, oral contraceptive pill (sometimes it helps acne), corticosteroids [Figure 8], isoniazid, and lithium [Table 1]. Recently, a new class of therapeutic agents - EGF-receptor antagonists (gefitinib, erlotinib, cetuximab) - have been recognized as a trigger of acneiform eruptions. [13],[14] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09234t1.jpg] [dv09234f8.jpg] [dv09234f7.jpg] [dv09234f6.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}