 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
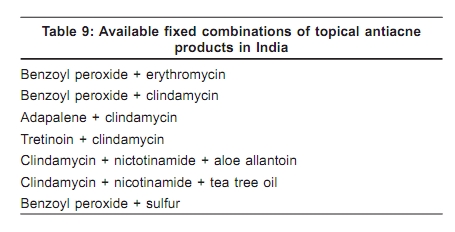
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 34 Acne in India: Guidelines for management - IAA Consensus Document Combination therapy Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09239 With the availability of different topical antiacne agents targeting different pathogenetic factors, it makes sense to combine them to enhance therapeutic efficacy, to make therapy more user-friendly, to minimize adverse effects, and to prevent or reduce bacterial resistance. This has been achieved through loose and fixed combinations. Topical retinoids in combination with topical or oral antimicrobials have been proven to reduce acne lesions, both comedones and inflammatory, faster and to a greater degree than antimicrobial therapy alone.[1] Together they target three out of four pathogenetic factors, namely: ductal hypercornification, P. acnes colonization, and inflammation. [1] Further, topical retinoids, through a thinning effect on stratum corneum, facilitate percutaneous penetration of topical antibiotics, and help achieve higher concentrations of the antimicrobial agent in the pilosebaceous canal which P. acnes inhabits. [1] Several clinical studies have evaluated loose [2],[3] and fixed [4],[5] combinations. All studies have arrived at the same conclusion that combinations are more effective. It has been recommended that combination of topical retinoid and topical antimicrobial be employed early in the treatment of mild to moderate acne, and a combination of topical retinoid and systemic antibiotic in severe acne. [6] Combination topical therapy is quite popular in our country. Often we go overboard and mix topical agents with gay abandon. It is common to come across prescriptions where four or more topical agents are mixed with no indication of methodology, leaving it to the poor patient to figure it out! This is proof of our professional freedom. The problem is mainly with loose combinations where chemistry and compatibility need to be understood. We also have available an array of fixed combinations [Table 9], of which BPO plus erythromycin, BPO plus clindamycin, adapalene plus clindamycin, and tretinoin plus clindamycin conform to international practice. Recent market data from Europe and USA reveal that the prescriptions for fixed combinations have increased while those for BPO have declined, and the market curve for topical antibiotics is flat. [7] Fixed combinations offer therapeutic breadth and practical convenience. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09239t9.jpg] |
| |||||||||

{kind=link}