 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
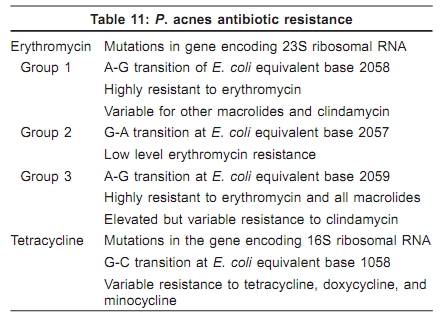
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 37-38 Acne in India: Guidelines for management - IAA Consensus Document Antibiotic resistance in acne Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09241 Antibiotic resistance is defined as a change in susceptibility of a microorganism to an antibiotic such that a higher concentration of the drug is required to inhibit growth of a resistant strain compared to fully susceptible wild type strain. Widespread use of tetracyclines and erythromycin occurred for more than 25 years before less-sensitive strains and clinically relevant or ′resistant′ strains were identified. In late 1970′s, a few strains of P. acnes that were relatively resistant to erythromycin and clindamycin were first reported and were viewed to be clinically not significant. [1] In the early 1980′s, shortly after the introduction of topical formulations of erythromycin and clindamycin, clinically relevant, less-sensitive strains were detected. [2] Some of these strains were highly resistant to erythromycin. Subsequently, in late 1980′s and early 1990′s, more clinically relevant antibiotic resistance and strains with multiple drug resistance were identified. [3],[4],[5] Generally, bacteria develop antibiotic resistance by acquiring plasmids, which can be transferred between strains of a species and even between species in some instances. With tetracycline and erythromycin, plasmids and transposons encode for pump proteins that efflux antibiotics away from ribosomes and, less commonly, the resistance is due to enzyme inactivation. [6],[7],[8] In case of clinically relevant strains of resistant P. acnes , plasmids have not been found. Rather, point mutations in the genes encoding the 23S rRNA (erythromycin) and the 16S rRNA (tetracycline) have been identified. [9],[10],[11],[12] Three phenotypes of erythromycin resistant P. acnes have been identified as shown in [Table 11]. It is important to know that microbiological resistance does not always equate with clinical resistance. Only concentration of the drug does not play sole role in controlling P. acnes colonization in the microenvironment of the comedone. Other local factors also contribute. Antibiotics also have direct anti-inflammatory actions. The concentration of antibiotics in pilosebaceous ducts varies considerably.[13] Various factors may be attributed to suboptimal antibiotic effects. For example, high sebum excretion rate may flush out antibiotic, thus lowering the concentration. Low concentration of the antibiotic favors emergence of antibiotic resistant P. acnes . Poor patient compliance is another factor that operates through lowered antibiotic concentration. When to Suspect Antibiotic Resistance ?
Treatment of Antibiotic Resistant Acne Options include using higher doses of the concerned antibiotics, for example, minocycline 100 mg b.i.d., doxycycline 100 mg b.i.d.; switching to another, previously not used, antibiotic, such as a newer macrolides, oral isotretinoin, and antiandrogens.
Can be overcome with higher doses. What is the magnitude of antibiotic resistance in acne in India is anybody′s guess? IAA believes it is high. If parallels can be drawn, than Spain, a country where prescription laws are lax much like our own, antibiotic resistance is the highest at 94%. [13] Every effort should be made to prevent antibiotic resistance. Global Alliance for Acne recommends that: antibiotics should not be prescribed unless necessary; treatment courses should be kept short; BPO should be combined with antibiotics or used in between antibiotic courses; simultaneous use of dissimilar oral and topical antibiotics should be avoided; and good compliance should be emphasized.
References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09241t11.jpg] |
| |||||||||

{kind=link}