 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
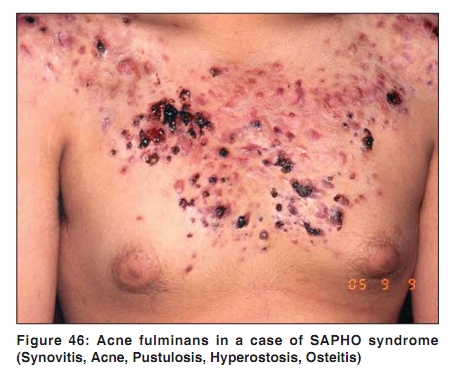
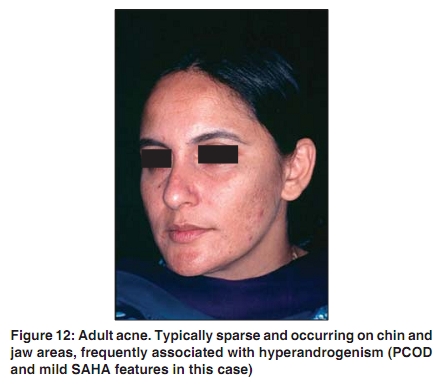
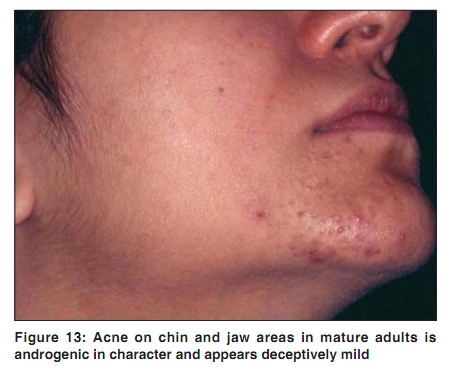
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 44-46 Acne in India: Guidelines for management - IAA Consensus Document Hormonal therapy of acne Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09243 Hormonal therapy is an excellent choice for female patients with acne who have SAHA syndrome [Figure 44],[Figure 45],[Figure 46], polycystic ovarian syndrome (PCOS), HAIR-AN syndrome (hyperandrogenism, insulin resistance, acanthosis nigricans) [Figure 50],[Figure 51],[Figure 52], or cutaneous hyperandrogenism (CH). It is also the logical treatment for adult/androgenic acne [Figure 12],[Figure 13] which is distinguished by its persistence or late onset, localization to the lower face, and premenstrual flares. Hormonal therapy is also justified in refractory/difficult acne and in nodulocystic acne where isotretinoin is either contraindicated or inadequate. Hormonal therapy is synergistic with other forms of acne therapy and may be combined to enhance therapeutic efficacy. [1] Hormonal therapy alone or in combination represents a higher step on the therapeutic ladder. Some hormonal therapies also provide contraception which can be a bonus. The goal of the hormonal therapy is to oppose the effects of androgens on the sebaceous glands and follicular keratinocytes. [1]
Hormonal evaluation in acne is indicated when cutaneous signs of hyperandrogenism are observed. These include, besides acne (vide supra), hirsutism, frontal scalp hair thinning, seborrhea, coarse facial skin with prominent ostia, acanthosis nigricans, and striae. About 50% of such individuals have underlying polycystic ovaries (bulky ovaries with loose stroma and multiple peripherally arranged follicles) and most of them are clinically identifiable by irregular menstrual cycle. The full syndrome with obesity, infertility, and insulin resistance is only occasionally seen in the dermatology clinics. PCOS is a spectral disease with mild and incomplete expressions. American College of Gynecologists (ACOG) criteria for clinical diagnosis of PCOS include: presence of anovulation (fewer than nine periods per year or periods> 40 days apart) and signs of hyperandrogenism. [2] CH is a clinical entity in itself and denotes absence of systemic features of hyperandrogenism. It is postulated that skin has the ability to synthesize androgens de novo. CH responds well to hormonal therapy. Hormonal evaluation is a prerequisite to hormonal therapy. A limited and budget-conscious evaluation should include LH, FSH, prolactin, total and free testosterone, DHEAS, and an ultrasound of abdomen and pelvis. While the ultrasound is best done on the second day of the cycle, blood hormone assays are recommended to be done in the luteal phase (last two weeks of the cycle). [1] Some experts prefer to do the blood hormone assays also on the second day. A comprehensive hormonal evaluation may also include cortisol AM and PM, androstenedione, 17-α-hydroxyprogesterone, 5-α-dihydrotestosterone, and sex hormone binding globulin. [1] LH/FSH ratio in excess of two supports PCOS. Modest elevation of prolactin and testosterone are likely ovarian in origin and part of PCOS. High levels of testosterone are uncommon and suggest ovarian tumor. DHEAS is derived from the adrenals. Modest increase is seen at adrenarche and its level correlates with the severity of comedonal acne in prepubertal girls. [3],[4] High levels of DHEAS indicate congenital adrenal hyperplasia (4000-8000 ng/ml), or adrenal tumor (over 8000 ng/ml). [1] Congenital adrenal hyperplasia (CAH) is also identified by elevated 17-a-hydroxyprogesterone. There are partial forms of CAH and the defect is 21 carboxylase and 11 carboxylase deficiencies [Figure 51]. Hormonal assays are expensive to perform and the cost of comprehensive hormonal evaluation is in excess of INR ten thousand.
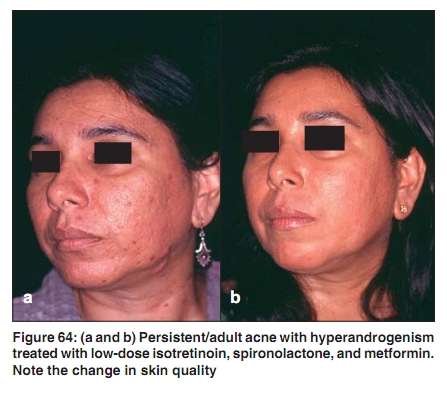
Specific hormonal therapies may be divided into two groups. One group is agents that block androgen receptors - also referred to as antiandrogens. This group includes cyproterone acetate, spironolactone, drospirenone, and flutamide. The other group is agents that decrease the androgen production by ovaries and adrenals. This group includes oral contraceptives and glucocorticoids. [1] Combination oral contraceptives are the most widely used agents in the treatment of acne especially in our country. The most popular combination is ethinylestradiol 35 µg plus cyproterone acetate 2 mg (EE-CPA). Besides decreasing ovarian production of androgens, EE-CPA also increases SHBG which, in turn, binds free circulating testosterone. The product is cost-effective, widely available, and well received by the patients. EE-CPA comes in a strip of 21 tablets. It can be started on day 1 (if contraception is a requirement) or day 5 (if the date of the menstruation is to be maintained); the therapeutic response is the same either way. The dose is one tablet a day, best taken after dinner and the course is repeated after seven tablet-free days. EE-CPA is typically given for 6-12 months but may be given for 3 years or longer where well tolerated and needed. It is contraindicated in patients with personal or family history of thromboembolism, and should be used with caution and with greater justification in cases with family history of breast or uterine malignancies, in mature adults, in the presence of depression, hypertension, or other internal medical problems. It may be used in combination with oral antibiotics, oral isotretinoin, and other adjunctive therapy. The combination with oral antibiotics may compromise the contraceptive function of EE-CPA. Whether EE-CPA causes weight gain is debatable? A newer combination oral contraceptive containing EE 20 µg and drospirenone 3 mg is available and is indicated in patients intolerant to EE-CPA (including those who allege weight gain), and in mature adults. Drospirenone is a derivative of spironolacone. Oral contraceptives containing third-generation progestins (norgestimate) and EE have also been used in acne. [5] Second-generation oral contraceptive ethinylestradiol plus desogesterel helps regulate menstrual cycle but does not exert antiandrogenic effect. Cyproterone acetate 50 mg is an imported drug. It is available as a tablet and is supplied as a bottle of 50 tablets. Fifty tablets cost approximately INR thirty five hundred. It can be combined with EE-CPA for a greater therapeutic effect. It is given as 50-100 mg for first ten days of the EE-CPA cycle for 5-10 cycles. It is very effective and well tolerated. Occasionally, it may cause reversible increase in blood pressure. Spironolactone functions both as an androgen receptor blocker and an inhibitor of 5a reductase. [1] In doses of 50-100 mg twice daily, it has been shown to reduce sebum production and improve acne. [5] It is also effective in reversing female androgenetic alopecia. It is indicated in therapy resistant acne and in cases of CH. It may be combined with other therapies [Figure 64]. It is widely available, cost effective, and well tolerated. Adverse effects include menstrual irregularities and breast tenderness. In young otherwise healthy females, hyperkalemia and hypotension are nonissues. Flutamide is an androgen receptor blocker. In a dose of 250 mg twice daily, in combination with an oral contraceptive, it is very effective in the treatment of hirsutism. It is also effective in acne, [7],[8] but because of few case reports of fatal hepatitis, and because other safer options are available, it is not very popular. Calutamide is a new introduction and is claimed to be less hepatotoxic. Finasteride, on the other hand, is ineffective in acne, because it works by inhibiting 5a reductase type II, which is present in hair follicles but not in sebaceous glands. Finasteride inhibits 50-60% of DHT, where as dutasteride, a newer compound, inhibits 90%. There are yet other agents with marginal antiandrogenic effect, namely: ketoconazole, cimetidine, and oral zinc. Zinc reportedly inhibits 5a reductase. [9] In conclusion, antiandrogens and oral contraceptives are effective and useful modalities in management of difficult and complicated acne, but because of their systemic effects, they should be used by dermatologists who are familiar with reproductive endocrinology, or those who elect to work with gynecologists or endocrinologists. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09243f64.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}