 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
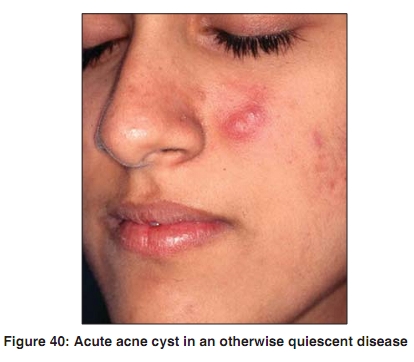
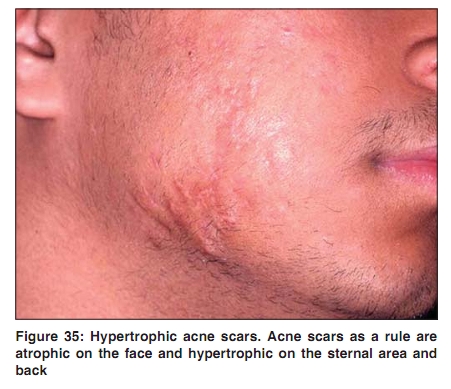
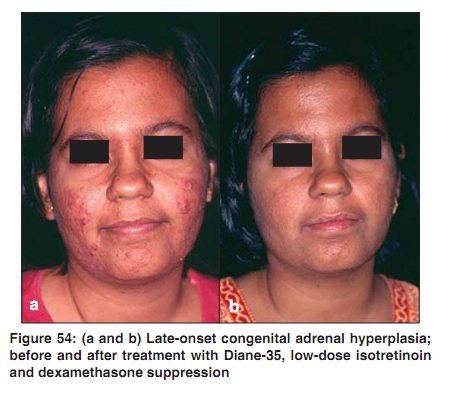
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 47-48 Acne in India: Guidelines for management - IAA Consensus Document Adjunctive therapies Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09244 Adjunctive therapies provide therapeutic width, which is often needed to enhance efficacy, limit dosages of primary agents to curtail toxicity (even costs!), and to help individualize treatment programs. In acne therapy several options are available: Corticosteroids: Oral, topical, and intralesional steroids are useful in different settings as supportive therapy for acne. Potent topical steroids may be used for short periods (7-10 days) to ameliorate severe inflammation, as in acne nodules, to achieve rapid clinical improvement that is often requested by the patients to meet social obligations. This simple therapeutic maneuver also minimizes the risk of subsequent scarring. The same can be achieved with intralesional triamcinolone (ILT) 2.5-5 mg/ml. ILT is faster and more effective, and prevents steroid abuse. ILT is an important treatment for persistent acne nodules and cysts [Figure 40] and quantities of 0.1-0.25 ml may be injected in the center of each lesion. [1] ILT is also indicated in the management of hypertrophic and keloidal acne scars [Figure 35], where it is injected in concentration of 10-20 mg/ml repeatedly at monthly intervals. [2] In severe forms of acne - nodulocystic acne, acne conglobata, and acne fulminans, and in acne flares evoked by other systemic therapies [Figure 45] - oral prednisolone in a dose of 0.5-1.0 mg/kg is a useful adjunct and may be prescribed for 2-3 weeks and tapered off over another 2-3 weeks.[3] Some of us prefer to use oral triamcinolone, 4-8 mg/day for 2-4 weeks. Low dose oral methylprednisolone, 4 mg on alternate nights, is recommended for cases of late-onset congenital adrenal hyperplasia [Figure 54], usually for six months. [4] Prednisolone 2.5-5 mg, or dexamethasone 0.25-0.75 mg at bedtime may also be used to suppress adrenal androgen production. [5] Oral Zinc: Chance observations of improvement in acne in patients of acrodermatitis enteropathica being treated with oral zinc in 1970′s led various workers to try zinc in acne vulgaris. Zinc inhibits chemotaxis and tumor necrosis factor-a production, and induces superoxide dismutase, besides inhibiting 5a-reductase. [6] In a randomized comparative study, it was found that 30 mg/day of oral zinc was only 17% less effective than minocycline (100 mg/day) in reducing inflammatory lesions. [7] The beneficial effect of zinc is independent of zinc deficiency. [7] In earlier studies, Michaelsson et al . [8] found zinc to be beneficial in acne vulgaris while Weimer et al . [9] did not find zinc to be better than placebo except that zinc appeared to have some-what beneficial effect on acne pustules. A recent case report suggests that oral zinc sulfate may be useful in dissecting cellulitis and acne conglobata.[11] Overall, the role of oral zinc in acne vulgaris seems questionable. Dapsone: Dapsone is an antimicrobial agent used in the treatment of leprosy. Its anti-inflammatory properties have led to its use in a wide variety of dermatologic disorders including acne vulgaris. In an uncontrolled study of 484 cases of acne of varying severity treated with dapsone 300 mg weekly, a dramatic response was reported; 80% regression of lesions at three months was observed in grade-IV acne. [11] Another study reported 75% improvement in nine of eleven patients in eight weeks of commencing dapsone at a dose of 300 mg weekly. [12] Yet another study compared 100 mg daily dapsone with 13-cis retinoic acid in the treatment of nodulocystic acne. [13] A significant improvement in all clinical parameters was observed in patients treated with 13-cis retinoic acid while only marginal clinical benefit was observed with dapsone. [13] In India, oral dapsone may be a worthy consideration in pustular acne in poor patients. Vitamin A: It is required for the maintenance of differentiated epithelia and mucus secretion, and is also necessary for correcting defects in keratinization in a number of skin diseases including acne vulgaris. Oral and topical vitamin A has been reported to improve and significantly modify acne. [14] A recent study has revealed that plasma concentration of vitamin A is lower in acne patients and this correlates with severity of the disease. [15] Vitamin A is retinol, and is the progenitor of retinoids. From the time it was learnt that 13-cis retinoic acid is sebosuppressive, vitamin A has also been used to treat acne with the same rationale as 13-cis retinoic acid, where retinoids were not available, or where there was resistance on the part of the patient to take retinoids. Some of us have used vitamin A extensively, typically in a dose of 50,000 units twice daily with vitamin E 400 IU, for 4-6 months. This combination has a therapeutic effect comparable to 20 mg of isotretinoin per day. The mucocutaneous effects are less, the costs are lower even at the current low price of isotretinoin, and for patients who read the fine-print of package inserts vitamin A is more acceptable. Vitamin A should not be used concomitantly with isotretinoin. Other drugs: A host of miscellaneous drugs have been used in acne over the years. Clofazimine and nonsteroidal anti-inflammatory drugs (NSAIDs) are anti-inflammatory options and have been used in acne fulminans. Anxiolytics and antidepressants may have a role in emotionally labile acne patients. There are anecdotal reports claiming usefulness of antihistamines and pyridoxine in preventing premenstrual flares of acne. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}