 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
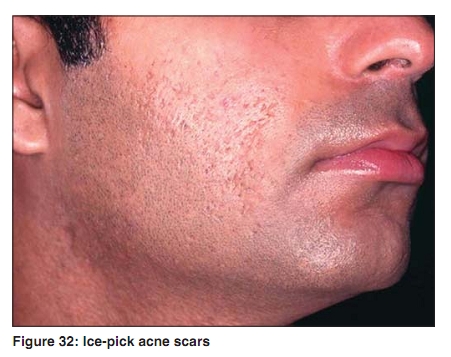
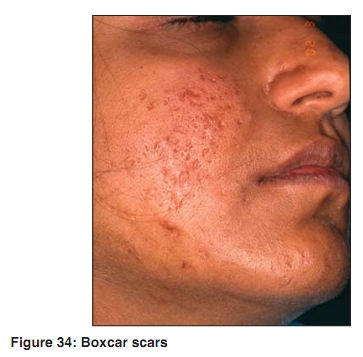
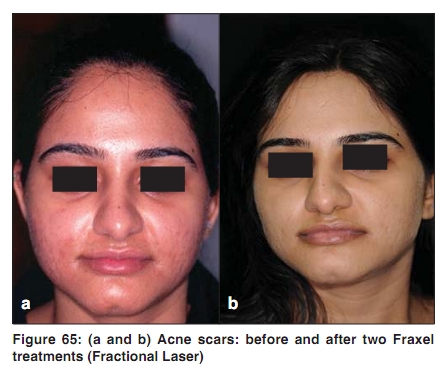
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 52-53 Acne in India: Guidelines for management - IAA Consensus Document Acne scars Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09247 Clearance of scars is the first request of the acne patients. There is lack of data on the epidemiology and pathophysiology of acne scars. There is limited data on clinical characteristics and management. There is often discrepancy between patient′s perception of scars and dermatologists assessment. In a survey of acne patients, 49% reported having scars. [1] In a clinical study in which acne scars were looked for by a dermatologist, 14% of the examined females, and 11% of the males were found to have them. [2] In another study, it was documented that 95% of the acne scars occurred on face, and there was no gender difference.[3] However, acne scars on the trunk were more common in males. [3] There was correlation between the severity of scars and delay between onset of acne lesions and start of acne treatment. [3] Genetic factors have an impact on predisposition to scarring, and type of scarring. [4],[5] Keloids on black skin have been linked to chromosomes 2q23 and 7p11. [5] Acne scars are determined by severity of inflammation as judged by depth and duration. Epidermal damage manifesting as erythema and pigmentation is reversible, while dermal damage as atrophic scars is partially reversible and hypertrophic scars not at all. Remodeling of collagen, the last step in tissue repair, is modulated by MMPs, which cause the damage, and tissue inhibitors of metalloproteases (TIMPs), which contain the damage. When the ratio of MMPs/TIMPs is low, atrophic scars occur and, conversely, when the ratio is high, hypertrophic scars occur. [6] Acne scar classification: Classification of acne scars [Table 4] is essential to assess the severity of cosmetic disfigurement and to choose the therapeutic intervention necessary. Broadly, acne scars are classified as atrophic and hypertrophic. Atrophic acne scars have been further classified as ice-pick, rolling, and boxcar [Figure 32],[Figure 33],[Figure 34]. [7] The European acne group (ECCA) has renamed the atrophic acne scars as V-shaped (ice-pick), U-shaped (boxcar), and W-shaped (rolling). [8] Scar characteristics can be further assessed with specialized techniques such as silicon elastomer mold which is then examined under a light microscope. Treatment of acne scars: Several approaches have been developed but as atrophic scars are the most common and face is the priority area, they are directed toward atrophic scars. Surgical techniques: Punch excision of ice-pick scars is easy and gives good early result; occasionally there is secondary widening. [9],[10] Punch autograft is used when treating deep ice-pick scars. The donor site is usually postauricular skin. Subcision involves subcutaneous sectioning of dermal adhesions with a sharp needle (1.5 inch, 18 Gauge, Nokor). It is often associated with neocollagenosis, and the technique is good for V, U, and W scars. [11] Resurfacing techniques: These include TCA peeling, phenol peeling, microdermabrasion, laser abrasion, selective thermolysis with Fraxel laser, and resurfacing by radiofrequency and electrosurgery. [9],[10] The objective is to restore skin contour by inducing neocollagenosis. Resurfacing is indicated in U and W scars. The main complication is erythema which persists for weeks. There is also risk of pigmentation. Spot TCA peeling is a good technique for V and deep U scars. A sharp stick (toothpick) soaked in 62% or 100% TCA is brought in contact with the target and the contact is maintained till whitening appears. It is a painful procedure and multiple sessions are required. In a study by Lee et al . [12] 62% TCA gave good results in 82% versus 94% with 100% TCA. Microdermabrasion: This involves planing of the skin by mechanized means utilizing the projection of micromarbles consisting of aluminum oxide on scars. Six to seven sessions, at two week intervals are needed. In one session, twenty passes are made on each area until superficial bleeding appears. Six to seven session microdermabrasion has low efficacy and may be useful in superficial U scars. [13] Chemabrasion is when microdermabrasion is combined with a peeling agent. Lasers: These are increasingly being used to treat acne scars. Intense Pulse Light (IPL) acts by heating the dermis and stimulating neocollagenosis. It has weak activity and may be helpful in red, hypertrophic scars. Light-Emitting Diode (LED) does not warm but acts by photomodulation. It is a safe and painless procedure but the efficacy is low. It is being used for superficial U scars, erythema (acne macules), and pigmentation. Ablative laser resurfacing, although effective, is associated with excessive tissue reaction as erythema and edema, and complications such as pigmentation and scarring. It is less suited for skin types V-VI. Fractional photothermolysis, a new concept, using 1,550-nm erbium-doped fiber laser (Fraxel ® ) appears to be very promising. Fractional photothermolysis creates microscopic thermal wounds to achieve skin rejuvenation without significant side effects. [14] In a study from USA, 53 patients (skin types I-V) with mild to moderate atrophic facial scars were treated with three treatment sessions at monthly intervals. Clinical improvement averaged 51-75% in nearly 90% of patients. Clinical response rates were independent of age, gender, or skin type. Side effects included transient erythema and edema in most patients, but no dyspigmentation, ulceration, or scarring. It was concluded that atrophic scars can be effectively and safely reduced with 1,550-nm erbium-doped fiber laser.[15] Fractional thermolysis (Fraxel ® ) is now available in some centers in India [Figure 65]. It is, however, an expensive treatment. The cost per treatment is INR 15-25,000 per sitting, and typically 4-8 sittings are required depending on the depth of scars. A single treatment with Fraxel ® in Singapore costs US$ 1000 (Dr CL Goh, personal communication), and US$ 1500 in Boston (Dr JS Dover, personal communication). Fillers: The aim is to lift the depression caused by scars, by injecting a filler underneath. There are several options. Resorbable filler such as hyaluronic acid is a good option. It lasts for 6-12 months. It is expensive but safe. It is indicated for scars with gentle slopes and no sclerosis. Nonresorbable fillers carry the risk of granuloma formation. Autologous fat transfer is another option. Dermabrasion: Dermabrasion using a motorized diamond head is becoming obsolete. It is a higher risk procedure with prolonged down-time and considerable risk of pigmentary disturbances. It has always been viewed as unsuitable for darker skin types, especially those residing in tropical areas. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09247f65.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}