 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
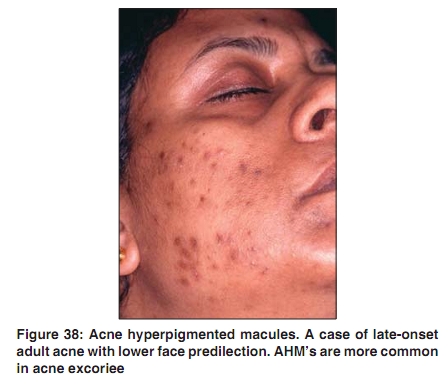
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 54 Acne in India: Guidelines for management - IAA Consensus Document Postinflammatory hyperpigmentation in acne Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09248 Postinflammatory hyperpigmentation (PIH) is a common sequela in acne patients, more so in those with skin of color. [1] PIH in acne is also called acne hyperpigmented macule (AHM). [1] AHM′s were noted in 65.3% of blacks, 52.7% of Hispanics, and 47.4% of Asians in a study of acne in the USA. [1] Such data are not available for acne patients in Indians but PIH is believed to be equally common in our patients [Figure 38]. PIH appears as a discolored macule, typically in shades of brown and black, depending on the skin type and the depth, but may also express as pink, red, or purple. [2] As the term implies, PIH reflects an acquired increase in cutaneous pigmentation induced by inflammation. This acquired excess pigment may be present in the epidermis, dermis, or both. [2] Cutaneous inflammatory response results in release and subsequent oxidation of arachidonic acid to prostaglandins, leukotrienes, and other products. These products of inflammation alter the activity of both immune cells and melanocytes. In the epidermis, the effect is stimulation of melanocytes, with consequent increase in the synthesis of melanin and its transfer to the keratinocytes. In the dermis, the excess melanin is derived from pigmentary incontinence resulting from incidental damage to the melanocytes residing in the basal layer. Dermal melanin is phagocytosed by macrophages (melanophages). [2] PIH occurs in areas of acne papules, pustules, and nodules, and its severity correlates with the severity of the inflammatory process and the underlying propensity based on the skin type. Squeezing and popping the acne lesions may contribute to PIH. Unlike acne scars, PIH is reversible. However, it may take months (3-24 months) to resolve spontaneously. The greater the contrast between the pigmented macule and the natural skin tone, the longer is the time taken for it to fade. PIH in acne is atleast partially preventable, and this can be done by containing inflammation with timely and judicious treatment, and by sun protection. Serious treatment of PIH in acne can only be initiated after the disease has remitted. However, modalities like topical azelaic acid and topical retinoids [3] can be incorporated during the active stage. For sun protection, regular use of a noncomedogenic, oil-free, sunscreen product with an SPF of 15 or greater is recommended. Topical treatments for PIH: There are several ways to approach this. The excess pigment can be bleached, new pigment formation can be blocked, the shedding of pigment by exfoliation can be accelerated, or a combination of the above. For bleaching excess pigment, various topical products containing hydroquinone, kojic acid, azelaic acid, retinoids, and steroids are employed. Diacneal, a retinaldehyde and glycolic acid combination cream is a new introduction for PIH in Europe. [4] For accelerating the exfoliation, options include topical products containing alpha hydroxy-acids, and chemical peels with glycolic acid, trichloracetic acid, or salicylic acid. Nontopical treatments for PIH: Microdermabrasion and nonablative lasers have been tested in PIH in acne with no clear conclusions as to their efficacy. The decision to employ such modalities depends on complex considerations involving availability, expertise, and the degree of desperation. References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology |
| |||||||||

{kind=link}