 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
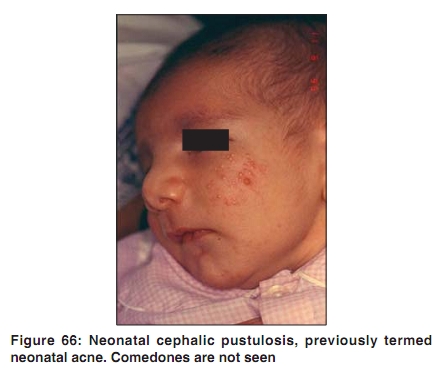
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 7, , 2009, pp. 57-58 Acne in India: Guidelines for management - IAA Consensus Document Acne in children Raj Kubba, AK Bajaj, DM Thappa, Rajeev Sharma, Maya Vedamurthy, Sandipan Dhar, S Criton, Rui Fernandez, AJ Kanwar, Uday Khopkar, Malavika Kohli, VP Kuriyipe, Koushik Lahiri, Nina Madnani, Deepak Parikh, Sudhir Pujara, KK Rajababu, S Sacchidanand, VK Sharma, Jayakar Thomas - members Indian Acne Alliance Correspondence Address: Dr. Raj Kubba, Consultant Dermatologist, Kubba Clinic, 10, Aradhana Enclave, Ring Road, New Delhi - 110066, India. rajkubba@hotmail.com Code Number: dv09250 Acne can be seen in the first year of life, early childhood, prepubertal age, and puberty. [1] However, in mid-childhood, between 1-7 years, acne is uncommon, and when it is encountered it should be evaluated for hyperandrogenism. [2] There are several subsets in childhood acne. Neonatal acne: It is actually not acne. It has been renamed as neonatal cephalic pustulosis (NCP). It presents in new borns, in the first few weeks of life, as papules and pustules on the cheeks, chin, eyelids, and forehead [Figure 66]. [1] Comedones are absent. NCP represents follicular or poral colonization with Malassezia sympodialis and M. globosa. [3] It is usually self-limiting and does not require any treatment. Infantile acne: It is less common than NCP and starts later, typically between 3-6 months. Boys are more frequently affected than girls, and there is usually a family history of severe acne. [4] The clinical picture shows the usual mix of acne lesions - comedones, inflammatory lesions including nodules and cysts, and in some cases, even scars [Figure 67]. The severity and course varies. Typically it remits between 1-2 years of age. If antibiotics are required, the choice is between erythromycin and trimethoprim (unavailable in India). Oral isotretinoin is indicated for nodular/scarring infantile acne. [5] Isotretinoin administration in young children is complicated because it is only available in gelatin capsules and is inactivated when exposed to sunlight and oxygen. [5] It is suggested that capsules should be opened in dim light and mixed with butter and jam and spread on a bread slice. [5] A second suggestion is to freeze the capsule to a solid consistency and then cut the capsule to the desired dose and conceal it within a palatable food such as a candy bar. [5] Mid-childhood acne: In mid-childhood between 1-7 years of age, acne is very rare. Clinically it is similar to infantile acne, but denotes hyperandrogenism. The best screening test for hyperandrogenism in this age group is bone age. [2] Prepubertal acne: It represents early adrenarche and may appear as early as eight years of age. It is more frequent among girls. [1] It is predominantly comedonal and central part of forehead is where it begins [Figure 9]. It is associated with raised levels of DHEAS and, in some cases, free testosterone. [1] It evolves into common acne and continues as adolescent acne. The treatment depends on the type and severity of lesions, and the age at treatment. Macrolides are the treatment of choice. Tetracyclines may be given above the age of eight years, although some experts draw the line at 10 years. Cephalexin is an option in the below 8-years age group. [6] References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09250f67.jpg] [dv09250f66.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}