 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
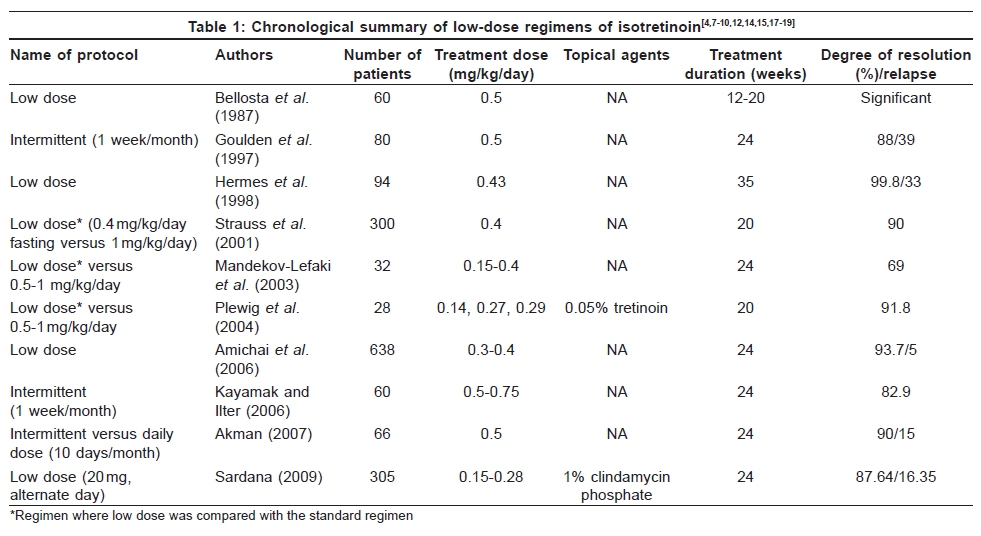
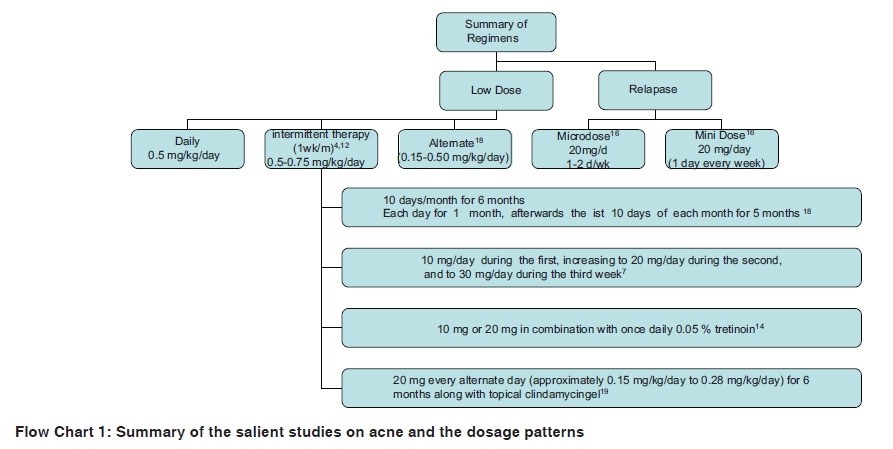
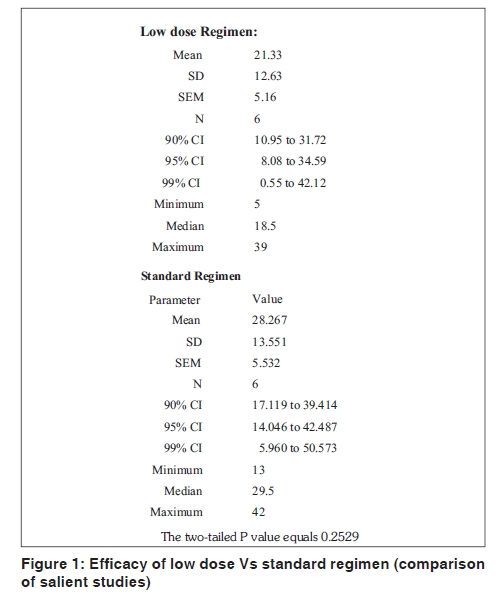
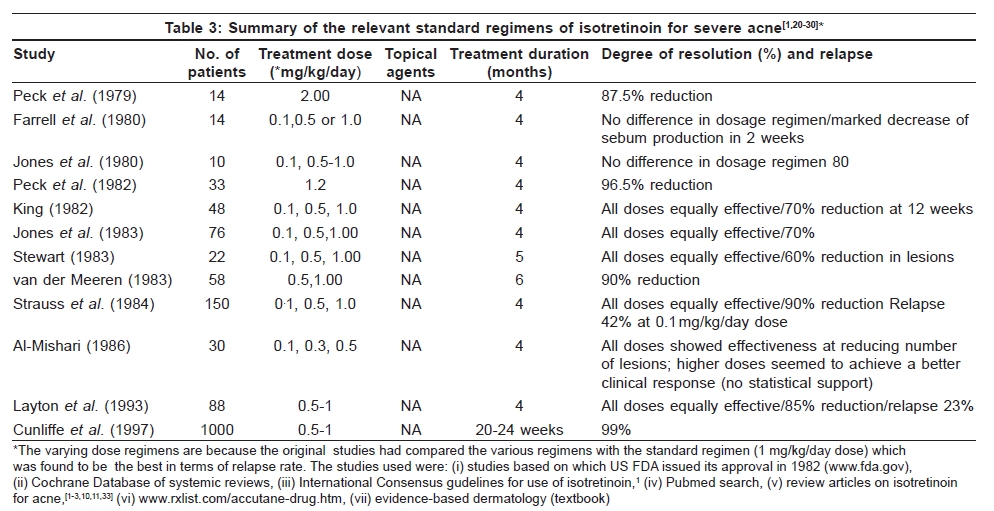
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 7-13 Review Article Efficacy of low-dose isotretinoin in acne vulgaris Kabir Sardana, Vijay K. Garg Department of Dermatology, Maulana Azad Medical College, Delhi, India Code Number: dv10003 PMID: 20061724 DOI: 10.4103/0378-6323.58672 Abstract Low-dose isotretinoin (0.5 mg/kg/day) is a mode of therapy for mild to moderate grades of acne.We analyzed the various trials of this mode of therapy with or without combination with topical agents.We also statistically analyzed the results, efficacy and relapse rates of standard therapy in comparison with the low-dose therapy. Our analysis of the data revealed that the efficacy and relapse rates of low-dose isotretinoin in mild to moderate grades of acne is comparable with the standard regimen (1 mg/kg/day), which is given in the severe grade of acne vulgaris. Thus, the grade of acne vulgaris should dictate the dose of administration of isotretinoin and the standard dose of 1 mg/kg/day is an unnecessary overtreatment for mild to moderate grades of acne.Keywords: Low-dose isotretinoin, acne vulgaris, efficacy Introduction Isotretinoin is an FDA approved drug for the treatment of severe cases of nodulocystic acne. [1] Its conventional recommended dose has been 0.5-1.0 mg/kg body weight per day for 16-32 weeks, with a maximum cumulative dose of 120 mg/kg. [1],[2],[3] It is used as an off-label indication for other grades of acne but erroneously in the same dose (1 mg/kg/day; cumulative dose of 120 mg/kg). This regimen is known to produce good results; however, it might cause several dose-dependent side effects. In an endeavour to surmount this limitation and to make the regimen cost-effective, low-dose regimens for mild/moderate grades of acne have been advocated. [4],[5],[6],[7],[8],[9] Interestingly, low-dose isotretinoin was attempted initially for severe acne also, [10],[11] with or without combination with other agents. In severe acne, lower doses of 0.3 or 0.5 mg/kg/day proved to be equally effective as the standard 1 mg/kg/day dose, [10],[11] but the high relapse rates were instrumental in discarding its use in severe acne. Recent studies have reinforced the view that low-dose isotretinoin is useful for mild to moderate acne [4],[5],[6],[7],[8],[9],[12] with less side-effects (cutaneous, systemic and laboratory based) as compared with the standard regimen. [11],[13],[14],[15],[16],[17],[18],[19] To compare the efficacy and relapse rate of standard versus the low-dose therapy, we analysed all the studies of low-dose isotretinoin in acne vulgaris with the studies of standard dosage leading up to the US FDA approval in 1982 and the international consensus guidelines of 1997. [1] The statistical analysis was performed using Graph Pad Analysis and the comparison of efficacy and relapse rate between standard therapy (1 mg/kg/day) and low-dose therapy was performed using the Mann-Whitney test (Unpaired t-test, non-parametric). Low-Dose Isotretinoin An analysis of the studies revealed that there were two broad categories of studies; in one in whom relapse occurred after standard treatment [5],[6],[16] and the other group where a low dose was given at the outset (daily/alternate day regimen) [4],[7],[8],[9],[10],[12],[14],[15],[17],[18],[19] [Table - 1] and [Table - 2]. Low-dose isotretinoin (regimens) Conventional low-dose therapy [Table - 1], [Flow Chart - 1] Low-dose isotretinoin has been used to treat acne by various authors. [4],[7],[8],[9],[12],[14],[15],[17],[18],[19] in various doses, like daily, [7],[17],[18] intermittent therapy, [4],[12],[18] alternate day therapy [19] or gradually increasing the daily dose. [5] As there is marked heterogeneity in these regimens, a more logical way is to compare them on the basis of dose per day (mg/kg/day), which ranges from 0.14 mg/ kg/day to 0.75 mg/kg/day. [4],[7],[8],[9],[10],[12],[14],[15],[17],[18],[19] Except for one study, [12] low-dose isotretinoin was uniformally of a dose less than 0.5 mg/kg/day. A different approach is the use of low-dose isotretinon in a micronized form, which pharmacologically has a similar efficacy to the conventional standard regimen of 1 mg/kg/day. This entailed the use of a formulation of micronized isotretinoin [17] in a single dose of 0.4 mg/kg/day isotretinoin regimen, which had been found to be of similar efficacy to the standard regimen of 1 mg/kg/day. Micro/mini dose [Table - 2] Another mode of administered isotretinoin is for cases of acne in adult patients or those who relapse after having received standard therapy of isotretinon. Palmer et al. [6] studied the effects of low-dose isotretinoin administration for 1 or 2 days of each week in adult patients suffering from a relapse. They used 20 mg/ day isotretinoin on eight adult patients with moderate acne who showed signs of recurrence within a few weeks after the treatment was discontinued. Amichai et al. [16] similarly treated 12 female patients with 20 mg of isotretinoin weekly for up to 3 years for relapses that developed between 6 months and 2 years after full-dose isotretinoin treatment with excellent results. Another special scenario is a very small number of patients who suffer from acne even in the sixth and seventh decades. [5] These are patients of persisting acne and have often received multiple courses of antibiotics over many years. Nine patients were treated with oral isotretinoin 0.25 mg/kg per day for 6 months; in six, the acne had virtually cleared by 3-4 months while in the other three it cleared by 6 months. On stopping the therapy after 36 months, the patients remained clear of acne except for one who relapsed after 11 months. [5] Pathological correlates A comprehensive analysis of the pathological correlates was performed with respect to sebum estimation, bacteriological analysis and biopsy evaluation by Plewig et al. [14] A study population of the acne conglobata group treated with 20 mg daily isotretinoin led to a reduction of the inflammatory lesion by 87-94%, non-inflammatory lesions by 81-88%, [14] reduction of the sebaceous gland size by 35-58%, sebum production by 90-95%, follicular keratinization by 55-70% and Propionibacterium acnes by 33-73%. [14] A low dose (5 mg/d -, 2.5 mg/d, or 2.5 mg 3x weekly) was also observed to reduce the sebum production by up to 64% and acne lesions by 84%, with a concomitant quantitative reduction of Propionibacterium acnes. [15] These results in acne and in seborrhoea [14],[15] confirm the role of low-dose isotretinoin in altering the patho physiological correlates in acne. Epidemiological parameters No statistically significant correlations were found between patient age, sex, duration of disease, location and type of acne. Various types of acne (mild/moderate/severe) and different sites (face and/or trunk) have been treated successfully but with variable durations (6-9 months). [4],[5],[6],[7],[8],[9],[18],[19] Selection criterion The selection criteria in studies varied but generally included cases of predominantly facial acne of a mild to moderate grade. [4],[7],[8],[9],[11],[12],[13],[14],[18],[19] In one study, [4] a stringent criterion of a total acne grade < 1, inflamed lesion count < 20 and sebum excretion rate < 1.25 μg/ cm 2 / min was used. Cumulative dose The cumulative dose varies depending on whether a combination therapy or monotherapy is administered.The cumulative dosage varies form 21 mg/kg [4] to as high as 180 mg/kg. [7] An analysis of the cumulative dosages of the representative studies [4],[7],[8],[9],[14],[15],[16],[17],[18],[19] revealed a mean dose of 49.71 mg/kg (SD 22.76, 99% CI 17.82-81.60). The low cumulative dosage (38.4 mg/kg) in some studies can be explained by the concomitant topical combination therapy [19] administered contrary to studies where only monotherapy was administered (78.9 mg/kg [7] and 66.8-70.2 mg/kg [9] ). Another study where a combination with topical tretinion 0.025% was given also found an improvement with a remarkably low dose of isotretinoin (25-53 mg). [14] These differences between studies can be explained by the type of dosage (alternate day) and the proven anti-inflammatory and anti-bacterial property [10],[11],[14],[19] of concomitant topical agents. Other factors explaining the variable cumulative dosages include sites (facial and/or truncal [4],[11] ) and grade of acne studied (mild, moderate, severe). [4],[7],[10] A critical total dosage or a threshold total dose to prevent relapse has not been arrived at as yet. Side-effects The cutaneous side-effects were mild, [19] and only 5% of the patients had a moderate elevation of liver enzymes, with a slight increase of serum lipids in 6% of the cases. These are comparable to a recent study [9] of low-dose isotretinoin and lower than the conventional therapy (35% hyperlipidemia and 10% elevated liver enzymes). [11],[13] Results Efficacy Studies on acne rarely have similar acne classification schemes, nor do they have same protocols or are age and sex parameters and so it is difficult to compare the results in various studies. But, an analysis of the studies [Table - 1] reveals that due to the intrinsic superlative efficacy of isotretinoin [1],[10],[11] in acne, the efficacy is as high as 88.52%, and excluding one study [8] (69%), a mean of 90% efficacy is maintained. Thus, the comparative analysis can be logically based on the dose of isotretinoin discounting the varying protocols. Hermes et al. [7] (8.3 months; 10 mg/d up to 0.43 mg/kg) reported very good results in 62.8% and good results in 31.9% of the patients. Mandekou-Lefaki et al. [8] achieved excellent results in 68% and fair to good results in 31.2% (dose of 0.15-0.4 mg/kg/d; 8 months). This contrasts with another recent study (0.3-0.4 mg/kg/d for 6 months), which showed impressive results ranging from 92.6 to 94.8%. [9] In a study from India, [19] a low dose (0.15-0.28 mg/kg/d) lead to "clinically significant" results in 87.54% of the patients, including 68.20% "very good" and 19.34% of "good" results. In conclusion, the efficacy ranged from 69 to 99%, [4],[7],[8],[9],[12],[14],[15],[17],[18],[19] with no difference between the weekly and the daily/alternate day regimen. [18],[19] Combination therapy Although a combination therapy in acne is better, [10],[11] there is only one published study of low-dose isotretinoin with a topical agent (tretinoin), which proved to be better than monotherapy. [14] A recent study used topical clindamycin gel with low-dose (alternate day) isotretinoin, [19] which made more pharmacological sense than giving a topical retinoid with a systemic retinoid. [10],[11],[14] This regimen [19] of alternate dose isotretinoin in conjunction with topical clindamycin given at the outset showed an efficacy of about 87% [Table - 1]. This study reinforced the efficacy of this regimen but found that adding a topical antibiotic [19] to low-dose isotretinoin would affect the pathophysiology of acne more favorably than adding a topical retinoid. [14] Standard regimen Isotretinoin was approved for use in acne with an explicit indication for the treatment of severe recalcitrant nodular acne in 1982 by the US FDA. This followed the landmark study of Peck et al., 1979 and Peck et al., 1982. [20],[23] Further studies culminated in the consensus dose of 1 mg/kg/day and the cumulative dose of 120-150 mg/kg. [1],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30] Studies were performed using varying doses ranging form 0.1-1 mg/kg/day. [1],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30] Eight Randomised Control Trials RCTs compared various isotretinoin dosage regimens ranging from 0.1 to 2.0 mg/kg/day. [20],[21],[22],[24],[25],[26],[27],[30] All doses studied resulted in a significantly decreased number of lesions. However, no dose-related clinical response could be detected among the doses tested. Only one trial [30] reported (somewhat anecdotally) that higher doses of oral isotretinoin resulted in better clinical outcomes. However, no statistics were available to substantiate this claim. It was suggested that the low dose might be used for mild to moderate grades of acne but no formal recommendation was issued. Studies from 1982 to 1997 reiterated the existing facts. The relapse rate has been the focus of various studies [28],[29],[32],[33],[34],[35] and a nested study recently published found a relapse rate of 41%. [35] Low-dose regimens versus standard regimen Efficacy [Figure - 1] There are only three studies comparing the low-dose regimen with the conventional regimen, [8],[14],[17] which have found the low-dose regimen to have a comparable efficacy. To compare the studies apart from the three mentioned above, we compared the studies of low-dose isotretinoin therapy [Table - 1] [4],[7],[8],[9],[14],[15],[16],[17],[18],[19] with the studies of standard isotretinoin therapy (1 mg/ kg/day) [Table - 3] [1],[20],[21],[22],[23],[24],[25],[26] for efficacy and we found that the difference in efficacy of standard versus low-dose therapy (87.8 versus 88.52) was not statistically significant (the two-tailed P-value equals 0.4655). Thus, with regard to efficacy, low-dose therapy is as good as standard therapy. Relapse/failure rate [Figure - 2] We analyzed the studies of low-dose isotretinoin and the relapse rates were found to vary from 3.9 to 39% [4],[7],[9],[16],[18] The various factors that predispose to relapse are females, polycystic ovarian disease, [11],[18],[19] lower cumulative dose, [1],[8],[10],[11],[19] acne on the back, [19] seborrhea and high pretreatment acne count. [4] The conventional regimen has a variable relapse rate of 22-30%. [1] Importantly, the relapse rate depends on the duration of the follow up, varying from short (38%) to long-term follow-up (41%). [27],[31] A comparison of the relapse rates of standard isotretinoin therapy (1 mg/kg/day) [1],[26],[27],[28],[29],[30],[31] versus the studies on low-dose isotretinoin therapy [4],[7],[8],[9],[14],[15],[16],[17],[18],[19] revealed that the difference in the mean relapse rate of standard versus low-dose therapy (34.6 versus 21.478) was not statistically significant (the two-tailed P-value equals 0.095). Thus, low-dose therapy has a relapse rate comparable with that of the standard therapy. Conclusions The problem that is faced in analyzing the trials of isotretinoin (low dose /standard) is that there are varying study designs, ranging from open to double blind trials, the acne classification used are not uniform, the age, sex and sites treated are variable and the dose administered and the duration is not uniform. But, a uniform feature in all studies [5],[6],[7],[8],[9],[10],[12],[13],[14],[15],[16],[17],[18],[19] is that low-dose isotretinoin constitutes a dose less than 0.5 mg/ kg/d [[Table - 1] and [Table - 2]; [Flow Chart - 1]. It can be given in any regimen (daily, alternate day or intermittent) [Flow Chart - 1] for a duration varying from 6-7 months and the side effects are less than that of standard therapy. On analyzing the efficacy, it was found that except for one study [8] (69%), a mean of 90% efficacy was maintained in spite of the heterogeneity of the study groups. Apparently, the long-acting repository action of isotretinoin effectively neutralises the variation in trial interventions. As the gold standard for therapy in acne for severe acne is isotretinoin in a dose of 1 mg/kg/day, we compared the low-dose regimen results with the standard regimen. The efficacy and relapse rates were found to be comparable and thus the low-dose therapy (0.5 mg/kg/day) can be effectively administered in patients with mild to moderate acne. Moreover, giving a standard dose of 1 mg/kg/day in cases of mild/moderate-grade acne is pharmacologically erroneous, consequentially causes more side-effects and is potentially open to medico-legal scrutiny as it is not an approved indication of the US FDA. The only issue to be resolved is to arrive at a cumulative dose of low-dose isotretinoin to prevent relapse. Long-term follow-up studies after clinical resolution in patients on low-dose isotretinoin might shed some light on this issue. But, as the relapse rates of standard isotretinoin are still high (23-41%), [32],[33],[34],[35] it is unlikely, in view of the stringent advisories of the US FDA on isotretinoin, that an early consensus can be arrived at on a relapse-free cumulative dose. [Figure - 3 Multiple Choice Questions] References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10003t1.jpg] [dv10003f1.jpg] [dv10003fc1.jpg] [dv10003t3.jpg] [dv10003f3.jpg] [dv10003f2.jpg] [dv10003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}