 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
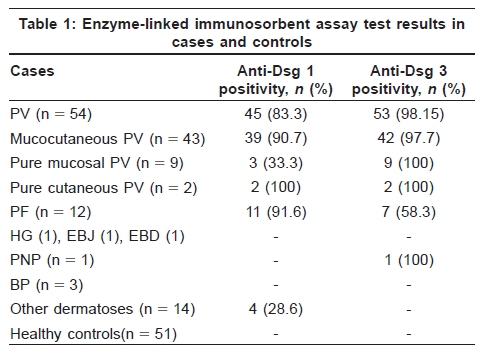
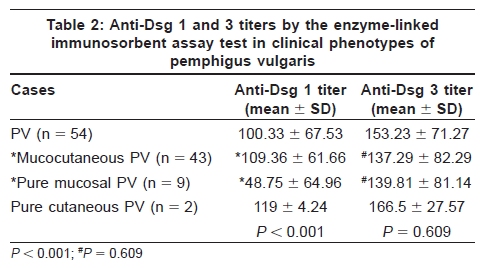
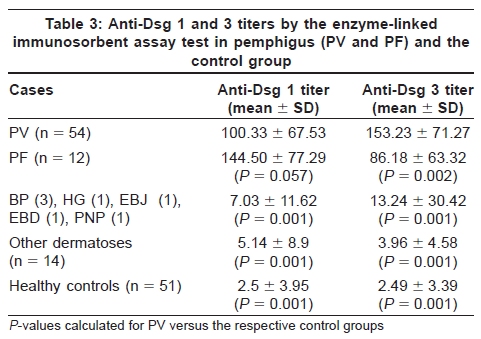
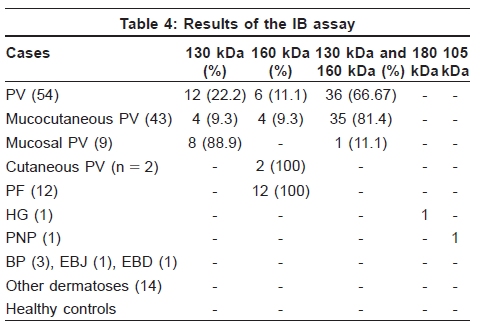
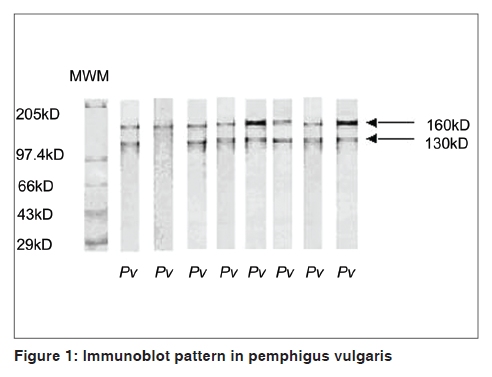
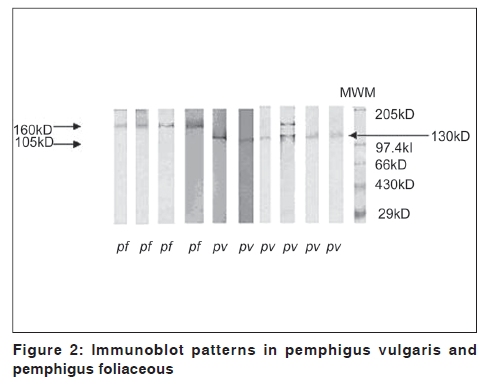
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 27-32 Original Article Comparison of enzyme-linked immunosorbent assay test with immunoblot assay in the diagnosis of pemphigus in Indian patients Sujay Khandpur, Vinod K. Sharma, Alpana Sharma1, Gaurav Pathria1, Abhigyan Satyam1 Department of Dermatology and Venereology, and Code Number: dv10006 PMID: 20061727 DOI: 10.4103/0378-6323.58675 Abstract Background: The diagnosis of pemphigus vulgaris (PV) and pemphigus foliaceous (PF) rests upon clinical, histological and immunofluorescence features. Enzyme-linked immunosorbent assay (ELISA) test and immunoblot (IB) assay have shown variable sensitivity and specificity. Aims: We compared the utility of ELISA and IB in pemphigus patients. Methods: Sixty-six pemphigus cases (PV-54, PF-12) and 72 controls (other vesicobullous disorders and healthy controls) were inducted. ELISA for anti-Dsg 3 and 1 antibodies and IB assay were performed. Results: On ELISA, both mean anti-Dsg 1 and 3 titers were raised in PV and PF. Mean anti-Dsg 1 in mucocutaneous PV was significantly higher than in mucosal PV and mean anti-Dsg 3 was significantly raised in PV than in PF. Anti-Dsg 1 and 3 in the control group were negative. Sensitivity and specificity of ELISA in PV was 98.14% and 90.5% while in PF it was 91.6% and 61.1%, respectively.On IB in PV, 36 cases (66.67%) showed the 130 kDa and 160 kDa antigen bands, 12 (22.2%) only the 130 kDa and six (11.1%) only the 160 kDa band. Eight of the nine pure mucosal cases (88.8%) showed only the 130 kDa. In PF, only the 160 kDa antigen was detected. These antigens were not identified in the control group. Sensitivity and specificity of IB in PV was 88.9% and 100% and in PF it was 100% and 95.2%, respectively. Conclusion: Both tests could differentiate pemphigus from other dermatoses, including other blistering disorders. ELISA could not make a distinction between PV and PF or between the various clinical phenotypes of PV. IB differentiated between PV and PF and the different clinical variants of PV. Keywords: Enzyme-linked immunosorbent assay test, immunoblot assay, pemphigus vulgaris, pemphigus foliaceous Introduction Pemphigus is a relatively common autoimmune blistering disorder involving the skin and mucous membranes. In a majority of the cases, the diagnosis of pemphigus vulgaris (PV) and pemphigus foliaceous (PF), the two major variants, rests upon clinical, histological and immunofluorescence features. [1] However, at times, differentiation between these two variants, between pemphigus and other vesicobullous disorders or between mucosal PV and other causes of oral ulceration is a diagnostic challenge. Direct immunofluorescence (DIF) shows a similar fluorescence pattern in PV and PF while indirect immunofluorescence carries the disadvantage of requiring animal substrates and shows substrate-dependent sensitivity, is a qualitative and subjective test and entails serial serum dilutions for its interpretation. Advancements in the field of immunology and molecular biology have revealed that Dsg 3 (130 kDa) and Dsg 1 (160 kDa) antigens, which are members of the cadherin superfamily of cell-cell adhesion molecules, are involved in PV and PF, respectively. The enzyme-linked immunosorbent assay (ELISA) test, based on the detection of circulating antibodies against recombinant desmoglein antigens produced in the Baculovirus system, has shown variable sensitivity and specificity in the diagnosis of pemphigus in different studies. [2],[3] Immunoblot (IB) assay has been utilized for the detection of pemphigus antigens from various sources, such as human epidermal extracts and bovine desmosomal preparations. [4] We undertook this study to identify the pemphigus antigens in Indian patients by IB assay, assess and compare the utility of ELISA test and IB assay in the diagnosis of PV and its various clinical phenotypes and differentiate PV from PF. Methods The study was undertaken between 2004 and 2006 (2 years) and was approved by our institute's ethics committee. All subjects gave written informed consent for participation in the study. We included 54 cases of PV and 12 of PF, diagnoses confirmed by histopathology (PV showing suprabasal acantholysis and PF showing subcorneal cleft). DIF was also performed in all cases. PV was divided into three clinical phenotypes depending on the localization of blisters and erosions at the time of presentation: Mucocutaneous, showing both mucosal and cutaneous erosions and blisters; pure mucosal, presenting with only mucosal erosions; pure cutaneous, presenting with only cutaneous blisters and erosions. Pure cutaneous PV was differentiated from PF histologically by the presence of suprabasal cleft in the former and subcorneal split in the latter. We took 72 controls, including other vesicobullous disorders (n = 7; bullous pemphigoid-3, herpes gestationis-1, epidermolysis bullosa dystrophicans-1, epidermolysis bullosa junctionalis-1 and paraneoplastic pemphigus-1), other dermatoses (n = 14, erythema multiforme, herpes zoster, varicella zoster, aphthous ulcer) and healthy controls (n = 51). Sera were obtained from all cases and controls, coded for blinded testing and stored at 270 o C until the assays were performed. Methodology of enzyme-linked immunosorbent assay test ELISA was performed at 1:100 dilution of serum using kits purchased from Medical and Biological Laboratories Co. Ltd, Nagoya, Japan. The assay was performed using the manufacturer's instructions and an ELISA index value above the cut-off of 20.0 (as per the manufacturer's instructions) was considered positive for both anti-Dsg 1 and 3. Methodology of immunoblot assay Thin-split skin grafts were obtained from normal skin over the upper thigh of five controls to extract and identify pemphigus antigens. Separation of the epidermis from the dermis was carried out by the ethylene diamine tetraacetic acid (EDTA) method: Skin pieces were gently stirred at 4 o C for 48 h in phosphate buffer saline with 2 mM EDTA and 2 mM phenyl methyl sulfonyl fluoride (PMSF). The separated epidermis was extracted according to the method described by Labib et al. [5] Estimation of protein in the supernatant was performed by Bradford's method. [6] Once the epidermal proteins were isolated, sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) was performed for their separation. This was performed by Lammeli's method with 8% resolving gel and 6% stacking gel. [7] The protein was transferred onto a nitrocellulose membrane (NCM, Membrane Technologies Inc., India) at 20 V constant voltage overnight at 4 0 C (Towbin et al.). [8] Transfer of proteins from SDS-PAGE gels to NCM was followed by incubation of NCM with patient sera (1:40). It was then incubated with horse radish peroxidase-conjugated rabbit anti human IgG secondary antibody (Dako- Cytomation, Denmark) at a dilution of 1:500 and color was developed using 3,3'-diaminobenzidine. Statistical analysis ELISA titer values for anti-Dsg 1 and 3 were analyzed statistically by calculating the mean and standard deviation. The minimum and maximum values were taken as range in the respective groups. The mean anti-Dsg 1 and 3 titer values were compared between PV and PF using the Mann-Whitney test. Further, the specificity and sensitivity of the ELISA test and IB assay were calculated. Receiver operating characteristic (ROC) analysis was carried out to determine the discriminating ability of anti-Dsg antibodies between PV and PF. ROC analysis includes a plot of true positivity (sensitivity) versus false positivity (1-specificity) at each titer value. The area under the curve joined by the points in the plot gives the discriminating ability of the criteria being evaluated. An area of 50% or less is considered to be a chance or worse than chance discrimination. Naturally, the more the area under the curve the more the discrimination. Results Of 54 PV cases, 43 had mucocutaneous involvement, nine had pure mucosal PV and two had pure cutaneous PV. Enzyme-linked immunosorbent assay results Pemphigus vulgaris Of 54 cases, 45 (83.3%) showed raised anti-Dsg 1 titer while 53 (98.15%) had elevated anti-Dsg 3 titer [Table - 1]. Of nine pure mucosal PV cases, all had markedly raised anti-Dsg 3 titer while the anti-Dsg 1 titer was elevated in only three (33.3%) cases. In the mucocutaneous variant, 39/43 (90.7%) had raised anti- Dsg 1 titer and 42 (97.7%) also had raised anti-Dsg 3 titer. In the pure cutaneous variant, both the cases had raised anti-Dsg 1 and 3 titers. Mean anti-Dsg 1 and 3 titers were raised in all clinical phenotypes of PV, although the mean anti-Dsg 1 titer in the mucocutaneous variant was significantly higher than the pure mucosal group ( P < 0.001), with no significant difference in the anti-Dsg3 titer ( P = 0.609), being high in both the groups [Table - 2]. Pemphigus foliaceous In PF, the anti-Dsg 1 level was raised in 11/12 cases (91.6%) and Dsg 3 in 7/12 cases (58.5%), although both mean anti-Dsg 1 and 3 titers were very high [Table - 3]. On comparing with PV, the mean anti-Dsg3 titer was significantly higher in PV than in PF ( P = 0.002), but with comparable anti-Dsg 1 titer ( P = 0.057). ROC analysis on anti-Dsg 3 values for PV and PF was performed to ascertain the cut-off value in differentiating between these two diseases because the mean anti-Dsg 3 titer was higher than 20.0 in both the conditions. We observed that for 100% PV specificity, the value was 182.84. ROC for anti-Dsg 1 was not performed as this antibody is raised in both conditions and is not used to differentiate between them. Sensitivity and specificity of ELISA in PV was 98.14% and 90.5% and in PF was 91.6% and 61.1%, respectively. The overall accuracy for PV and PF were 93.7% and 61.5%, respectively. Control group The mean anti-Dsg 1 and 3 titers in other vesicobullous disorders, other dermatoses and healthy controls were negative [Table - 3]. Results of IB assay In PV, two types of patterns were observed [Table - 4], [Figure - 1] and [Figure - 2]. The majority of the cases, i.e. 36/54 (66.67%) showed two bands corresponding to the 130 kDa and the 160 kDa antigens, 12 (22.2%) showed only the 130 kDa while six cases (11.1%) showed the 160 kDa. Of the 43 mucocutaneous cases, 35 (81.4%) showed both the 130 kDa and the 160 kDa bands while four each (9.3%) showed either the 130 kDa or 160 kDa band. Eight of nine (88.9%) pure mucosal cases showed only a single band of the 130 kDa and both pure cutaneous cases demonstrated only the 160 kDa band. All PF cases showed only the 160 kDa band. In other vesicobullous disorders, other dermatoses and healthy controls, neither of the two antigens were identified. Sensitivity and specificity of this test in PV was 88.9% and 100% and in PF was 100% and 95.2%, respectively. The overall accuracy for both PV and PF was 95.7%. Discussion ELISA test is a simple, quick and quantitative diagnostic modality for pemphigus that requires a very small quantity of serum and a large number of samples can be analyzed together. Previous studies by Harman et al. and Amagai et al. have shown ELISA to be a good tool to differentiate between PV and PF. [2],[3] They proposed that a positive anti-Dsg 3 was suggestive of PV irrespective of the anti-Dsg1 titer, which was high in a large proportion of both diseases. In our study, this test could differentiate pemphigus (PV and PF) from other dermatoses. However, both anti-Dsg 1 and 3 titers were raised in all clinical phenotypes of PV and in PF. Hence, it could not make a distinction between PV and PF or between different PV variants. Anti-Dsg 1 values were raised in 33.3% of pure mucosal cases while Dsg 3 was high in all pure cutaneous cases, which suggests that the antibody profile is not the sole determinant of clinical manifestations. However, the mean anti-Dsg 1 titer was significantly higher in the mucocutaneous variant as compared with pure mucosal PV. Several human studies in PV and PF have shown that, although anti-desmoglein antibodies relate to the phenotype of PV and PF respectively and that their therapeutic removal is of clinical benefit, there are several evidences that antibody specificities and titer do not always relate to the clinical phenotype. [9] It has been suggested that appearance of Dsg 1 autoantibodies in PV may occur as a consequence of epitope spreading. [10] There is a strong evidence of intramolecular epitope spreading, with polyclonal Dsg-specific IgG antibodies in the patients' sera recognizing both pathogenic and non-pathogenic epitopes located in the ectodomains of Dsg 3 and 1. A significantly high frequency of anti-Dsg 1 antibody in PV has been reported among patients from the Indian subcontinent as compared with those of other races, suggesting that certain ethnic and geographic factors may also contribute toward the clinical profile of disease. [11] PV patients from various racial backgrounds have shown a common association with several alleles, including DRB1FNx010402,1401 and DQB1FNx010302,1503. It may be hypothesized that certain HLA alleles predispose to the development of anti-Dsg 1 and others to anti-Dsg 3 antibodies. In our previous study also we observed that the ELISA test could not differentiate between the various clinical phenotypes of PV because both anti-Dsg 1 and 3 titers were raised in all the three variants. [12] Jamora et al. reported a high anti-Dsg 1 titer in 28% of mucosal PV and its absence in 29% of the cutaneous variant. [13] Delmonte et al. reported raised anti-Dsg 1 antibody in 62% of PV. [14] In a Thai study, anti-Dsg 1 and Dsg 3 antibodies were found in 85.7% and 100% cases respectively in PV while in Iranian patients they were detected in 76.7% and 94.5% patients respectively. [15],[16] In PF, both mean anti-Dsg1 and 3 titers were high in our study. 91.6% cases had raised anti-Dsg1 titer while 58.3% showed anti-Dsg 3 positivity. In another Indian study, anti-Dsg 1 and 3 were raised in 83.3% and 16.6% PF cases, respectively. [17] Arteaga et al. demonstrated anti-Dsg 3 in 6.88% of PF cases and suggested that separate species of antibodies are present rather than one that are capable of cross-reacting with both Dsg-1 and 3. [18] Interestingly, they showed that these Dsg 3 antibodies when affinity purified and passively transferred into mice induced a PV-like skin disease. Hilario-Vargas and colleagues detected anti-Dsg 3 by ELISA in 43% of fogo selvagem cases and 20% normal subjects living in an endemic area. [19] None of them developed any obvious clinical phenotype of PV, such as oral lesions, probably because quantities of pathogenic anti-Dsg 3 were insufficient to induce the PV phenotype, as they found intensity of immunoprecipitated Dsg 3 weaker than Dsg 1, or it may be due to the epitope shift. In many studies, low titers of desmoglein antibodies have been detected in 15-48% of first-degree relatives of pemphigus patients by indirect immuno fluorescence (IIF). [20],[21] Kricheli et al. suggested that these antibodies were not high enough to bind pemphigus antigens and induce acantholysis. [21] These authors also found similar titers of PV IgG1-3 subclasses among patients and their relatives but PV IgG4 was higher in patients and lower in relatives. This finding may indicate the role of PV IgG subclasses in the pathogenesis. Moreover, although immunogenetic factors constitute important aspect in the pathogenesis of pemphigus, they are solely not determinants of disease and probably require interactions with genetic and environmental factors. We also compared the sensitivity and specificity of ELISA with the IB assay. The IB assay was performed using human epidermis obtained from split-thickness skin grafts. The EDTA method was used for dermo-epidermal junction (DEJ) separation, 2-mercaptoethanol for epidermal extraction of proteins and proteinase inhibitors that improved liberation of PV antigens made the antigenic bands clear, sharply defined and narrow, resulting in a very reliable and reproducible assay. Conventionally, adult foreskin obtained during circumcision surgery has been used as an antigen source. Despite our efforts, the thick preputial skin did not give us a good-quality epidermis; hence, we used ultrathin split-skin grafts. Some authors have also used suction blister roofs as a substrate to isolate pemphigus antigens. [4] In our study, the majority of the mucocutaneous PV cases showed both the 130 kDa and the 160 kDa antigens, in pure mucosal type only the 130 kDa and in pure cutaneous only 160 kDa antigen was recognized. Hence, these two variants could be differentiated by this test. This modality could also differentiate between PV and PF as only the 160 kDa antigen was identified in PF cases. The overall accuracy for diagnosis of PV and PF by ELISA was 93.7% and 61.5% respectively while by IB it was 95.7% in both the conditions. Hence, IB is a better diagnostic modality for PF than the ELISA test Pure cutaneous PV could not be differentiated from PF either by ELISA test (anti-Dsg 1 and 3 titers were raised in both conditions) or IB assay (only the 160 kDa antigen was detected in both disorders). In the control group, including other blistering disorders, these two antigens could not be isolated, which shows that this test is both very sensitive and specific in pemphigus. Other studies have shown variable results on IB assay depending on the tissue used for antigen isolation (human epidermal extract, bovine desmosomal preparations, keratinocyte cell culture) and technique of DEJ separation (heat, EDTA or dispase method) because certain procedures may destroy or mask particular antigens or use 2-mercaptoethanol for antigen extraction. [4],[22] Hashimoto (1990) reported that all PV sera reacted with the 130 kDa antigen while only 26% of the PF sera exhibited reactivity with the 150 kDa antigen in the human epidermal extract. [4] However, in the bovine muzzle preparation, 61.5% of PF sera identified this antigen. Another study in 1995 demonstrated reactivity of all PV sera to the 130 kDa antigen and only 50% reactivity of PF to the 160 kDa antigen. [23] On using bovine extracts, certain PV sera reacted with both 130 kDa and 160 kDa antigens. It was proposed that simultaneous reactivity with both the antigens was produced by different subsets of antibodies rather than by cross-reactivity of a single antibody. In the same year, Ohata et al. demonstrated 130 kDa in all and 160 kDa in addition in three PV cases. [22] The majority of the PF sera (71.4%) identified only the 160 kDa antigen. Joly et al. reported the reactivity of 66.67% of PV sera to the 130 kDa antigen and 50% reactivity of the Tunisian PF to the 160 kDa antigen. [24] We found the ELISA test to be a less expensive and time consuming test than the IB. In the present study, the ELISA test differentiated pemphigus from other disorders but not between PV and PF or between different clinical phenotypes of PV. The novel pattern of antigen involvement as demonstrated by the IB assay helped to differentiate between PV variants and also between PV and PF. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10006f1.jpg] [dv10006t4.jpg] [dv10006f2.jpg] [dv10006t3.jpg] [dv10006t2.jpg] [dv10006t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}