 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
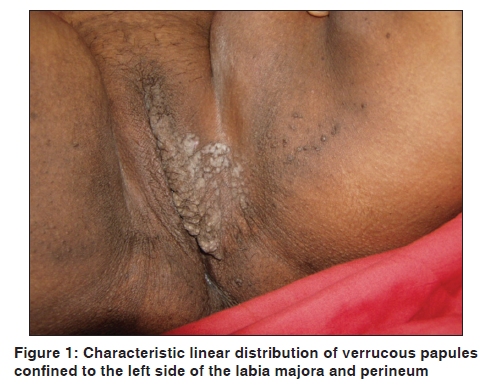
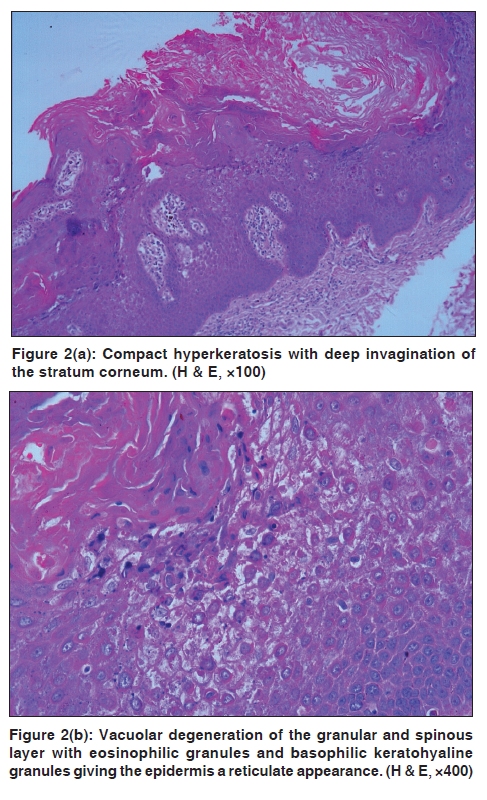
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 49-51 Case Report Linear epidermolytic acanthoma of vulva: An unusual presentation Molly Thomas, Renu George, Meera Thomas1 Department of Dermatology, Venereology and Leprosy, 1Department of Pathology, Christian Medical College and Hospital, Vellore, India Code Number: dv10010 PMID: 20061731 DOI: 10.4103/0378-6323.58679 Abstract Epidermolytic acanthoma (EA) is a rare benign tumor that shows epidermolytic hyperkeratosis (EH) on histopathology. It can occur in a solitary or disseminated form. This condition needs to be distinguished from other hereditary or acquired conditions that may show EH. We diagnosed an unusual case of EA of the vulva presenting in a linear pattern in a 50-year-old lady based on the clinical features and typical histopathological findings and stress the importance of considering epidermolyic acanthoma in the differential diagnosis of verrucous lesions of the genitalia.Keywords: Acanthoma, epidermolytic, linear, vulva Introduction Epidermolytic hyperkeratosis (EH) is an abnormality of epidermal maturation characterized by compact hyperkeratosis, accompanied by granular and vacuolar degeneration of the cells of the spinous and granular layer. It is associated with solitary or widespread cutaneous diseases of an inherited or acquired nature. [1] Among the acquired conditions, epidermolytic acanthoma (EA) is unusual and can present as a warty lesion in patients of all ages in solitary, spreading or disseminated forms. We report an unusual case of linear EA of the vulva occurring in a 50-year-old lady. EH localized to the female genitalia are rare and so is the linear type of EA. There have been no reports till date, to the best of our knowledge, of a linear type of EA of the vulva. Case Report A 50-year-old lady from Bangladesh presented to us with complaints of a mildly pruritic verrucous lesion on the left side of the vulva since early adulthood. It started off as a single papule on the left labia majora that gradually spread to involve a major portion of the left labia majora with extension to the thigh and perineum over a period of a few years. She had no other comorbidities nor any history of extramarital exposures. There was no family history of any ichthyosiform disorder. Cutaneous examination revealed a hyperpigmented linear greyish-white verrucous plaque involving the outer aspect of the labia majora on the left side. Few verrucous papules extended to the adjacent thigh and the perineum [Figure - 1]. The differential diagnoses considered were verrucae, condyloma acuminata, localized Darier's disease and inflammatory verrucous epidermal naevus. Light microscopy examination of skin biopsy specimen revealed compact hyperkeratosis, focal acanthosis and low papillomatosis with deep invagination of the stratum corneum. The granular and spinous layer showed vacuolization of cells with increased keratoyaline granules. The dermis was unremarkable [Figure - 2]a and b. On clinicopathological correlation, we arrived at a diagnosis of EA. Discussion EA, a benign acquired tumor of the epidermis, was first described in 1970 by Shapiro and Baraf when they reported six cases of solitary lesions and one case of multiple lesions (on the scrotum), which on histopathology showed thickening of the malpigian layer (acanthoma) associated with epidermolytic degeneration of the keratinocytes of the upper layers of the stratum spinosum and of the stratum granulosum. They gave it the name of acanthoma epidermolyticum. [2] The term EA is applied to discrete epidermal proliferations characterized by EH. EA has been described in different locations, namely eyelid, leg, anus, [2] abdomen, [3] back, [4] forearm, [4] scrotum [5] and the vulval region. [6],[7] In a majority of the reports, the lesions are solitary, but multiple lesions have also been described, especially in the scrotum [5] and vulva. [6] Disseminated lesions have also been well documented, [3],[4] especially in one patient associated with underlying immunosuppression due to kidney transplantation [4] where up to 100 lesions were present. Another clinical variant called multiple spreading type of EAs of genital and perigenital skin has been recently described in a male. [8] EH localized to the female genital area are rare. Few cases of female genital EH have been described involving the vaginal wall [6] and vulva, [7],[9],[10] but there have been no reports till date of a linear type of EA of the vulva as seen in our patient, limited to one side, in a linear pattern on the vulva with extension to the perineum and thighs. Dermatoses like psoriasis, lichen planus and lichen sriatus are some of the well-established acquired diseases exhibiting Blaschko's linear distribution. Because the clinical picture did not fit into any of the previous descriptions of solitary, spreading or disseminated forms of EA, in that it was confined to only one side of the vulva and was in a linear pattern, we propose the term "linear type of EA" for this particular pattern of clinical presentation that has not been previously described to the best of our knowledge. EH is an abnormality of epidermal maturation most commonly due to mutations in keratin 1 and 10, which may be congenital or an acquired defect. EH is an essential histologic finding in three hereditary skin diseases, i.e. bullous congenital ichthyosiform erythroderma, systemized verrucous nevus and hereditary palmoplantar keratoderma of Vorner. EH can be seen as an incidental finding in combination with distinct histopathologic features of few lesions like seborrhoeic keratosis, pilar cyst, cutaneous horn, actinic keratoses, leukokeratosis, intradermal nevus, malignant melanoma and lichen amyloidosis. [1] Many hypotheses have been postulated regarding pathogenesis of EA but none has been validated. Immunohistochemical techniques have shown that mutations in K1 and K10 gene may be a reason for the expression of this condition. [11] These keratins are synthesized by suprabasal keratinocytes during the differentiation of the epidermis. These mutations could be induced by numerous factors as UV radiation through intense sun exposure, [3] immunosuppression [4] or repeated trauma. [5],[8] Electron microscopy demonstrates that the mechanism of blister formation is cytolysis rather than acantholysis. [7] Attempts to isolate human papilloma virus DNA, in biopsies of EA cases, have been negative. [12] In our patient, repeated trauma due to itching could have been responsible for the localized spread of the disease to the surrounding area without any involvement of the opposite side, the vulva being a common site for neurodermatitis. The main differential diagnosis for EA in the genitalia include condyloma acuminata, localized Darier's disease and bowenoid papulosis, which can be clearly distinguished by histopathology. Neither the koilocytes characteristic of condyloma nor the acantholytic dyskeratosis of Darier's disease nor the characteristic keratinocytic atypia with the loss of normal polarity of bowenoid papulosis is seen in EA. The possibility of epidermolytic verrucous naevus was ruled out because the onset was in adulthood with gradual progression of lesions over a period of years. Our patient declined any further treatment once she was relieved to know the benign nature of the lesion. EA with vulval localization, although relatively uncommon, should be considered in the differential diagnosis of asymptomatic warty lesions in the genitalia. We propose that this clinical variant also be included in the clinical presentations of this rare benign epidermal tumor and emphasize the importance of histopathology in differentiating verrucous lesions of the genitalia. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10010f1.jpg] [dv10010f2.jpg] |
| |||||||||

{kind=link}
{kind=link}