 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
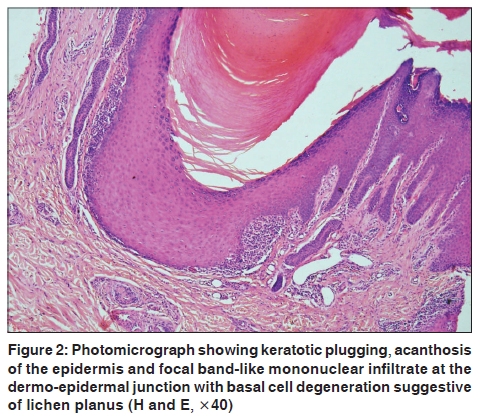
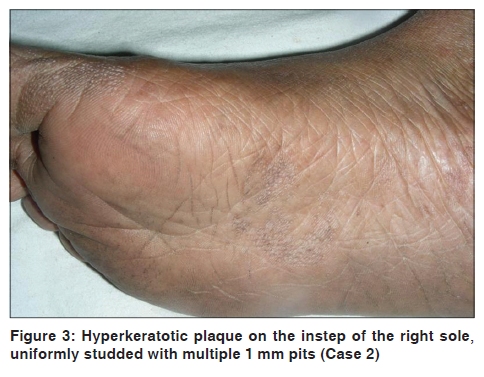
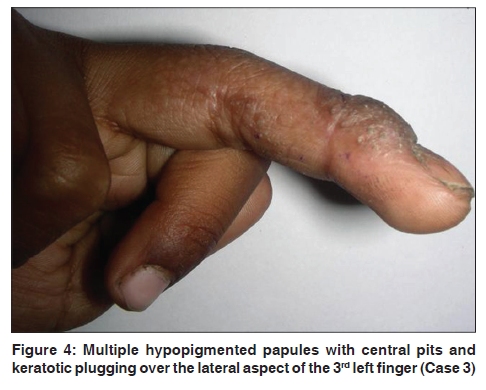
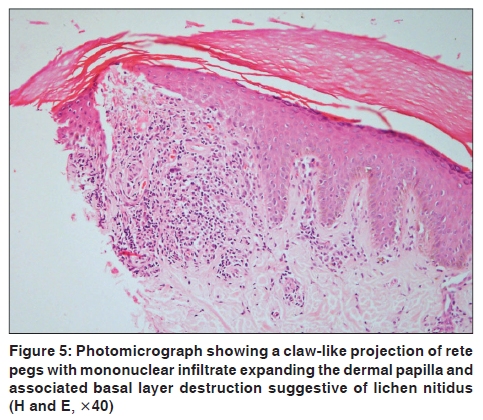
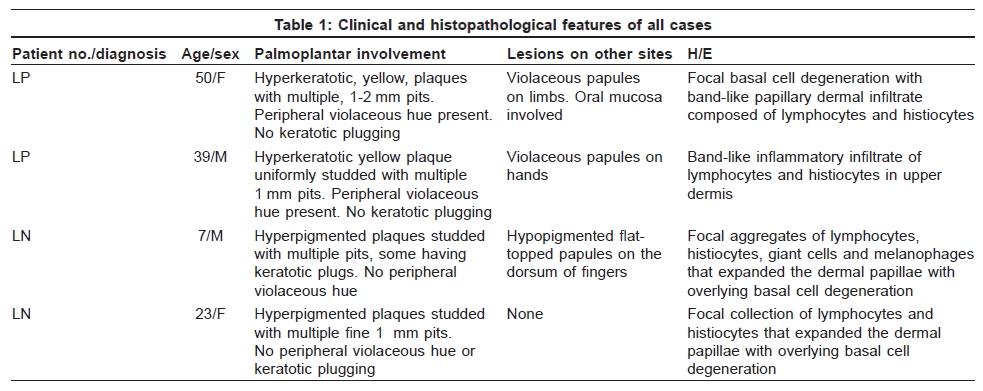
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 52-55 Case Report Hyperkeratotic pitted plaques on the palms and soles Sujay Khandpur, Sushruta D. Kathuria, Ruchika Gupta1, Manoj K. Singh1, Vinod K. Sharma Department of Dermatology and Venereology, 1Pathology, All India Institute of Medical Sciences, New Delhi 110 029, India Code Number: dv10011 PMID: 20061732 DOI: 10.4103/0378-6323.58680 Abstract Lichen planus (LP) and lichen nitidus (LN) present with varied morphology on the palms and soles. We present four unusual cases of palmoplantar LP and LN manifesting as hyperkeratotic plaques with pits. The diagnosis was confirmed histologically. Subtle features like presence of violaceous border suggests LP and plugs within the pits suggest LN.Keywords: Lichen nitidus, lichen planus, pits, palms, soles Introduction Variation in the morphology according to site is known in various diseases and is especially prominent on the palms and soles. Lichen planus (LP) and lichen nitidus (LN) are two such conditions where the palmoplantar lesions differ from classical lesions occurring at other body sites. [1] We present two cases each of LP and LN involving the palms and soles with an unusual morphology. Case Reports Case 1 A 50-year-old female presented with multiple violaceous, flat-topped papules and plaques of size 4 mm to 1 cm on the legs, feet, medial aspect of the thighs, interphalangeal joints and dorsa of the hands since 2 years. On the palms (both thenar and hypothenar eminence) and soles, there were well-defined, hyperkeratotic, yellowish plaques with peripheral violaceous hue. The plaques were studded with multiple, 1-2 mm pits [Figure - 1], which had fine white 1-2 mm scales. In the smaller papules, pits identical to those on the palms and soles were seen. Koebnerization was present. The oral cavity showed violaceous plaques with a lacy white pattern over the tongue. A biopsy from the palmar plaque showed keratotic plugging, focal basal cell degeneration with band-like papillary dermal infiltrate composed of lymphocytes and histiocytes, consistent with LP [Figure - 2]. She was treated with oral minipulse steroid therapy (5 mg of betamethasone on two consecutive days of the week) and topical clobetasol propionate ointment for 3 months with 30% flattening of the palmoplantar lesions. Case 2 A 39-year-old man presented with yellowish plaques on both soles with onset from the insteps since 7 years. Violaceous papules had developed over the dorsa of both hands since 2 months. He was a known hypothyroid controlled on L-thyroxine. On the instep of the right sole, there was a well-defined yellowish hyperkeratotic plaque uniformly studded with multiple 1 mm pits [Figure - 3]. Fine white scaling was present in the pits. On the left sole and on the left thenar eminence, multiple similar pits could be observed. Violaceous papules on the hands showed pitting. Examination of the oral cavity, hair and nails was unremarkable. Skin biopsy from the plaque on the right sole was consistent with LP. He was treated with a combination of topical clobetasol propionate and salicylic acid and, after 3 months, there was 60% flattening of the plaques. Case 3 A 7-year-old boy presented with multiple-grouped hypopigmented flat-topped papules on the dorsum of the right 2 nd to 4 th fingers and the left 2 nd and 3 rd fingers and hyperpigmented plaques studded with multiple pits, some having keratotic plugs, on the palmar aspect of the right 3 rd and 4 th fingers and proximal nail folds since 6 months [Figure - 4]. Few finger nails showed longitudinal ridging. Biopsy from the hyperpigmented pitted plaque showed focal aggregates of lymphocytes, histiocytes, giant cells and melanophages that expanded the dermal papillae with overlying basal cell degeneration [Figure - 5]. Biopsy from the hypopigmented papule showed the parakeratotic plug invaginating the epidermis with marked basal cell damage and a narrow band of lymphocytes and histiocytes. Histopathological features were compatible with LN. The child was treated with topical clobetasol propionate cream and after 3 weeks there was flattening of the lesions. Similar lesions developed on the right knee, which were treated similarly. Case 4 A 23-year-old woman presented with gradually progressive hyperpigmented plaques on the palms and the right wrist since 6 years. With a diagnosis of tuberculosis verrucosa cutis, she was treated for 20 months with antitubercular therapy without any response. On cutaneous examination, there was involvement of the right palm (both thenar and hypothenar eminences) and wrist and left palm and lateral aspect of the fingers with dark brown plaques studded with multiple fine 1 mm pits [Figure - 6]. There was fine white scaling within the pits. There was no violaceous hue or erythema in the plaques. Biopsy from the plaque on the palm showed features of LN. She was treated with a combination of topical clobetasol propionate and salicylic acid and after 2 months there was 40% flattening of the plaques. Clinical details of all four cases are described in [Table - 1]. Discussion The morphology of most dermatological conditions differ on the palms and soles, which makes clinical diagnosis in the absence of other cutaneous manifestations quite challenging. Palmoplantar involvement in LP and LN has been uncommonly described. [1] In a clinico-etiological study of 375 LP patients, involvement of the palms was seen in only 3.5% and of soles in 4.3% of the cases. [2] Various morphological patterns of palmoplantar LP have been described, including erythematous scaly plaques, yellowish hyperkeratotic papules, diffuse keratoderma, ulcerated lesions, vesicle-like papules and diffuse palmar hyperpigmentation. [3],[4],[5],[6] The internal arch of the foot and thenar and hypothenar eminences are common sites while fingertips are usually not involved. [3] An unusual presentation of palmoplantar LP, with involvement of bilateral palms, hypothenar and thenar eminences with hyperkeratotic, yellowish, coalescent papules with a violaceous rim and a central punctum and histologically showing lichenoid infiltrate has been reported. [7] The first two patients in our series demonstrated unusual morphology in the form of pitted hyperkeratotic plaques over the palms and soles. The coexistence of typical LP lesions elsewhere, including the oral cavity, and a representative histopathology helped clinch the diagnosis. Presence of violaceous hue at the periphery of the plaques has been described previously and may be considered a clue to the diagnosis. [3] Diagnosis of palmoplantar LN is usually suggested by monomorphic skin-colored tiny papules, similar to those seen at other sites. Rarer presentations include diffuse palmoplantar hyperkeratosis with fissuring occurring in the presence of typical lesions of LN elsewhere, minute keratotic spicules at the edge of diffuse palmoplantar hyperkeratosis, reddish brown keratotic papules on the dorsum and lateral borders of the hands and feet, keratotic papules with central depression, fine sandpaper-like hyperkeratosis and purpuric lesions. [8],[9],[10],[11],[12] Nail changes are common with LN in the palmoplantar region. [11] Our third and fourth cases showed hyperpigmented plaques with pits, which, on biopsy, showed features of LN. It has been suggested that the presence of plugs within the papules differentiates LN from LP. [13] In our series also, central plug was present in a case (Case 3) of palmoplantar LN. Arsenical keratosis, Darier's disease and nevoid basal cell carcinoma can also present with pitted papules and plaques, but these lesions are skin colored to yellowish and other cutaneous manifestations of the disease are present. [14] Other conditions with pitted palmoplantar papules and plaques include porokeratotic eccrine ostial and dermal duct naevus with linearly arranged lesions and hyperkeratosis punctata of the palmar creases that manifest as hyperkeratotic papules with central plugs restricted to the palmar creases. [15] We suggest that hyperkeratotic plaques with pits on the palm and soles are highly suggestive of lichenoid pathology and should prompt search for LP/LN at other sites. Presence of plugs within the pits is suggestive of LN and a violaceous rim indicates LP. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10011f4.jpg] [dv10011f6.jpg] [dv10011f3.jpg] [dv10011f2.jpg] [dv10011f1.jpg] [dv10011t1.jpg] [dv10011f5.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}