 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
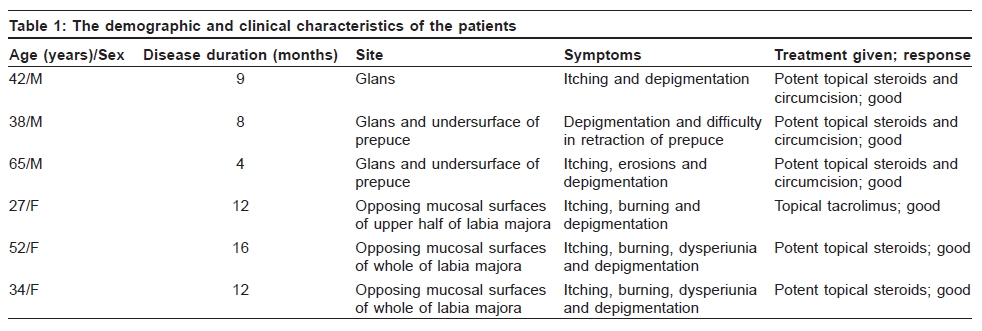
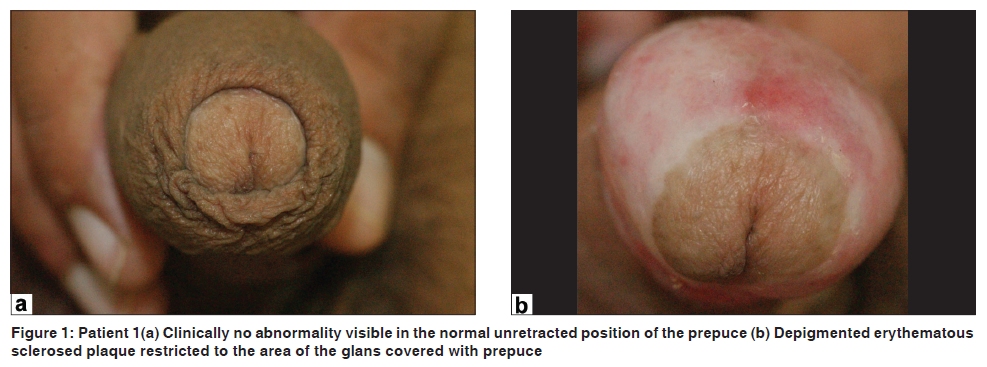
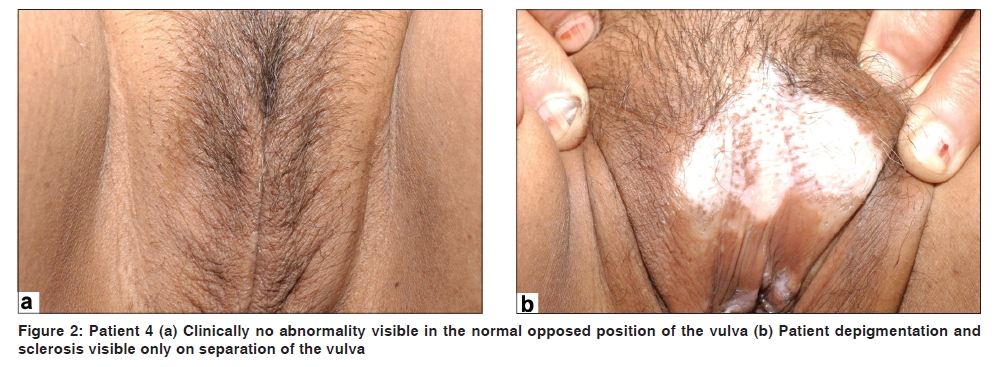
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 56-58 Case Report Lichen sclerosus: Role of occlusion of the genital skin in the pathogenesis Somesh Gupta, Amit Kumar Malhotra, Ajith C.1 Department of Dermatology and Venereology, All India Institute of Medical Sciences New Delhi - 110 029, 1Postgraduate Institute of Medical Education and Research, Chandigarh, India Code Number: dv10012 PMID: 20061733 DOI: 10.4103/0378-6323.58681 Abstract Lichen sclerosus (LS) is a chronic inflammatory skin disease, which most commonly involves the anogenital region. The etiology of LS is obscure, but genetic susceptibility, autoimmune mechanisms, infective agents like human papillomavirus and spirochaetes, and Koebner phenomenon has been postulated as causative factors. We report our observation in 6 patients (3 males and 3 females) with histologically proven lichen sclerosus that showed relative sparing of the uncovered areas of the genitals, thereby suggesting that the occlusion of the genital skin may be playing a greater role in the causation of LS than is currently thought, in both sexes.Keywords: Lichen sclerosus, role of occlusion, genitalia Introduction Lichen sclerosus (LS) is a chronic inflammatory skin disease, which most commonly involves the anogenital region. It is characterized by depigmentation and fibrosis leading to the intractable soreness, progressing eventually to destructive scarring.[1] The commonly involved sites on the male genitalia are meatus followed by prepuce, penile shaft and the glans penis. [2] A few experts consider LS of penis synonymous with balanitis xerotica obliterans (BXO),[3] but BXO may also be a consequence of other dermatoses that lead to fibrosis, such as cicatricial pemphigoid and lichen planus.[4] The etiology of LS is obscure, but genetic susceptibility including HLA A1, B8, DR3 association,[5] autoimmune mechanisms,[4],[6] infective agents like human papillomavirus[7] and spirochaetes,[8] and Koebner phenomenon[1],[4] have been postulated as causative factors. We report our observation in 6 patients (3 males and 3 females) with histologically proven lichen sclerosus that showed relative sparing of the uncovered areas of the genitals, thereby suggesting that the occlusion of the genital skin may be playing a greater role in the causation of LS than is currently thought, in both sexes. Case Report [Table - 1] shows the demographic and clinical characteristics of the patients. In males, the disease predominantly involved the inner aspect of the prepuce and the areas of the glans covered by the prepuce up to the preputial ring, with almost complete sparing of the exposed areas of the glans [Figure - 1]a and b. In females only the opposed surfaces of the vulva were predominantly affected [Figure - 2]a and b, in such a way that no abnormalities were visible unless the labia were separated manually. Discussion The prepuce is a penta-laminar specialized junctional tissue with mucosa on the inner surface covering the glans and the skin on the outer surface,[2] with preputial ring demarcating the two. This observation of involvement of the genital mucosa restricted to the opposing surfaces of the glans and the vulva suggests the role of occlusion in the development of genital LS. This hypothesis is further supported by the fact that in most cases of early LS of the penis, the preputial involvement is restricted to its mucosal side and the external surface of the prepuce is spared until later stages.[2] Similarly, in women with early genital LS, often the sclerosed depigmented area remains sharply confined to the opposing mucosal surfaces.[2] There are several possible mechanisms that may either alone or collectively, explain the effect of occlusion of the genital skin in the pathogenesis of LS. Studies have shown that LS is very rare in circumcised males. [4] The minor trauma induced by the foreskin in the uncircumcised males may be important in the initiation of the pathological process of LS due to koebnerazitation. Besides LS, many other inflammatory skin diseases such as psoriasis and lichen planus that manifest Koebner phenomenon are less common in the circumcised individuals.[4] Though the extent to which the minor trauma plays role in the pathogenesis of LS is not known. Also the presence of foreskin and poor hygiene facilitates the accumulation of smegma at the inner aspect of prepuce. The role of smegma as a predisposing factor in the development of carcinoma of the penis in the uncircumcised males has already been emphasized.[9] The same factor may also be contributing to the development of LS in uncircumcised males, since LS predisposes to malignancy[1],[9],[10] and both LS as well as carcinoma of penis are more common in uncircumcised males. Many cases of LS in the males remain undiagnosed as LS has been shown to be a frequent histological finding in males who have undergone circumcision for other indications.[4],[11],[12] In boys who are circumcised for phimosis and the histopathology shows features of LS, it is presumed that LS precedes and leads to phimosis. However, our observation raises a possibility that in some patients, opposite may hold true, where occlusion caused by longstanding phimosis may be leading to the development of LS. This pilot observation suggests that occlusion of the genital skin may be playing a greater role in the causation of LS than is currently thought. More studies on the causative factors of LS with emphasis on the role of preputial skin in males and vulval skin in females are necessary. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10012f2.jpg] [dv10012f1.jpg] [dv10012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}