 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
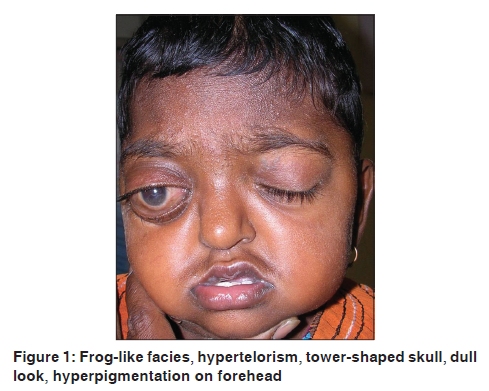
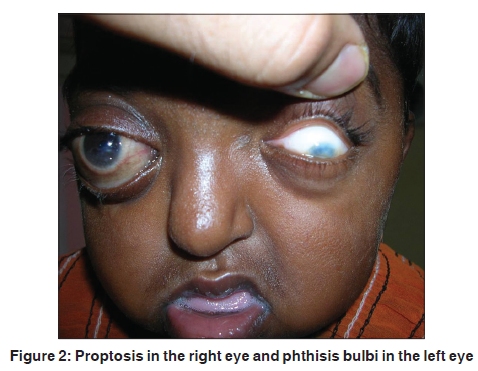
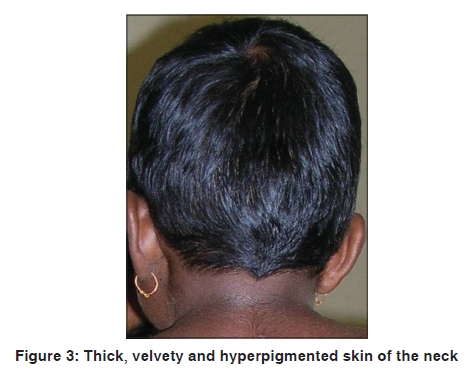
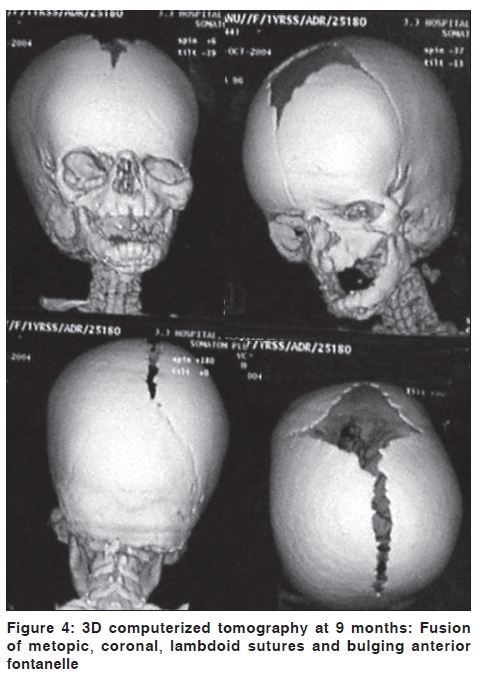
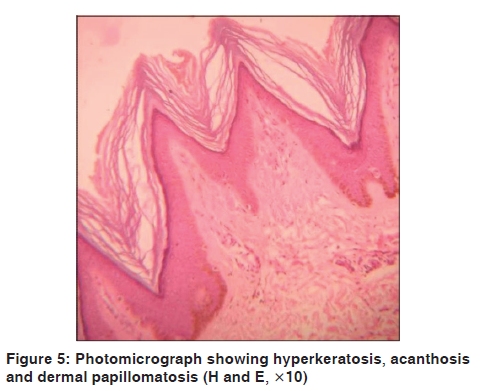
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 65-67 Letter to the Editor A rare association of acanthosis nigricans with Crouzon syndrome Ajay Kumar Gupta, Sankha Koley1, Sanjiv Choudhary1, Arvind Bhake2, Vikrant Saoji1, Atul Salodkar1 Departments of Ophthalmology, 1Dermatology and 2Pathology, J.N.M.C. Sawangi, Wardha, Maharastra, India. Code Number: dv10018 PMID: 20061739 DOI: 10.4103/0378-6323.58687 Sir, Crouzon syndrome was described in 1912 as one of the varieties of craniofacial dysostoses caused by premature obliteration and ossification of two or more sutures; most often, coronal and sagittal. It is caused by a mutation in the fibroblast growth factor receptor-2 (FGFR2) gene. Acanthosis nigricans can coexist with Crouzon syndrome. But, here, mutation is noted in the transmembrane region of FGFR3 (locus 4p16.3). [1] The combination of Crouzon syndrome with acanthosis nigricans is assumed to be a rare abnormality. Although the true frequency is uncertain, [2] some estimate that acanthosis nigricans is associated with 5% of all Crouzon cases. According to Friedhofer et al., [2] in 2006, only 30 cases of Crouzon syndrome with acanthosis nigricans had been reported in the medical literature. Because Crouzon syndrome is an autosomal-dominant disorder with variable expressions, history of consanguinity and family history are important. But, there are cases due to mutations. We report this rare association of acanthosis nigricans with Crouzon syndrome presenting with severe ocular complications in early childhood. A 5-year-old male child was presented in the ophthalmology outpatient department (OPD) with gradual bulging of the right eye. The patient was referred to the dermatology OPD for skin changes. There was no history of similar disorder in the family. There was also no history of consanguinity of marriage in the parents. The child was apparently normal at birth. The mother noticed a gradual bulging of the left eye after 3-4 weeks of birth. Gradually, there was expulsion of the left eye ball from the socket and rupture of the globe at the age of 3-4 months. When the child was 5-6 months old, she noticed a similar gradual bulging of the child's right eye for which she consulted a tertiary care center in Mumbai. Operative procedures were suggested but she did not visit for the next 3 months. On examination, the following features were noticed [Figure - 1] and [Figure - 2]: Frog-shaped facies, hypertelorism, proptosis and exposure keratitis in the right eye, phthisis bulbi in the left eye, irregularly shaped vault with left side of the head enlarged, mid-facial hypoplasia, mandibular prognathism, parrot beak-type of nose, high-arched palate and tower-shaped skull. The child was under weight (10.5 kg) with delayed developmental milestones. These findings were accompanied by thick, velvety and hyperpigmented skin involving the axilla, neck [Figure - 3], forehead, perioral area and eyelids (especially lower eyelids) [Figure - 1]. X-ray of the skull and 3D computerized tomography (CT) axial scan of the skull were carried out at the age of 9 months. Radiograph of the skull revealed a bulging anterior fontanelle with right orbit size larger than the left. A hammered-silver ('beaten metal/copper beaten') appearance was seen due to compression of the developing brain on the fused bones of the skull. 3D CT scan of skull revealed [Figure - 4] bulging anterior fontanelle. Craniosynostosis was seen with premature fusion of metopic, coronal and lamboid sutures. But, the sagittal suture lines did not fuse. The right side of the cranial fossae appeared smaller in size as compared with the left side. Histopathology of the skin biopsy taken from the neck revealed hyperkeratosis, acanthosis and papillomatosis [Figure - 5]. All patients with acanthosis nigricans and Crouzon syndrome, described in the medical literature, had an excess of skin and hyperpigmented lesions in the orbital area (predominantly on the lower eyelid), on the perioral area, neck and armpits. [2] Crouzon syndrome is due to a mutation of the gene (locus 10 q 26) for FGFR2. Acanthosis nigricans is a feature of several syndromes caused by active mutations of the FGFR3. [3] These include rare Crouzon syndrome with acanthosis nigricans, thanatophoric dysplasia, severe achondroplasia with developmental delay and acanthosis nigricans (SADDAN syndrome). These data support the view that the association of Crouzon syndrome with acanthosis nigricans is a different entity from the classic Crouzon syndrome. [4],[5] The disproportion between craniostenosis and brain growing may lead to death at a very early age. Early prenatal diagnosis can aid in diagnostic, therapeutic and further management in women who want to continue with pregnancy. Ultrasound in combination with medical history can be used to diagnose Crouzon syndrome in the second trimester of pregnancy.[6] A chorionic villus biopsy performed early in the 11 th gestational week of the first trimester can also diagnose this disorder by isolating the DNA. [7] Recent development of 3D ultrasonography and magnetic resonance imaging allow a more efficient early detection and diagnosis of fetal malformation. [8] Paucity of reports of Crouzon syndrome with acanthosis nigricans, especially in the Indian literature, prompted us to report this case here. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10018f4.jpg] [dv10018f2.jpg] [dv10018f1.jpg] [dv10018f3.jpg] [dv10018f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}