 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
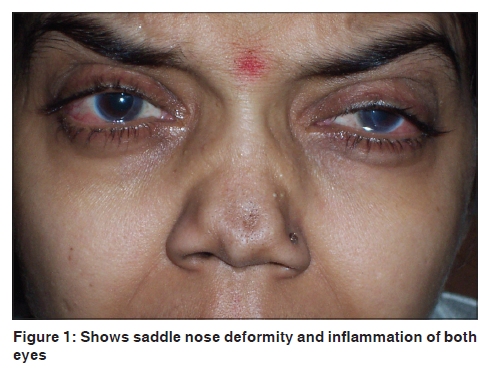
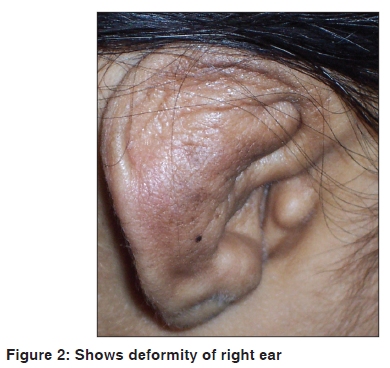
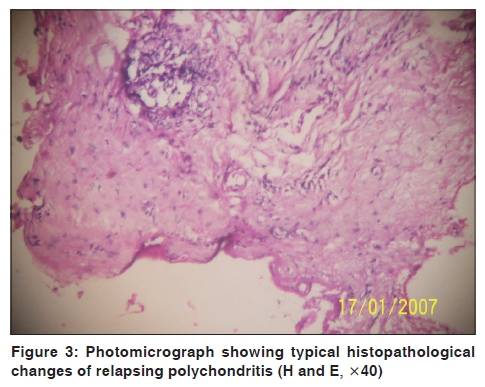
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 67-69 Letter to the Editor Relapsing polychondritis - delayed diagnosis and fatal outcome Krina Patel Department of Dermatology, Smt. S. C. L. Hospital, Smt. N.H.L. Municipal Medical College, Ahmedabad - 380 018, India Code Number: dv10019 PMID: 20061740 DOI: 10.4103/0378-6323.58688 Sir, Relapsing polychondritis (RP) is an inflammatory disorder, episodic in nature, characterized by recurrent inflammation of cartilaginous tissues and eventual destruction of affected tissues. The disorder mainly affects the eyes, respiratory tract, nose, and ears. It has a chronic relapsing and remitting course that can be fatal at times; although most times, it is the disfigurement due to tissue destruction that is of concern; rather than the threat to life. RP can present in a highly ambiguous fashion, and in one series of cases the mean delay from time of presentation to diagnosis was 2.9 years. [1] Criteria for the diagnosis, as suggested by McAdams and colleagues, include three or more of the following clinical features: (1) bilateral auricular chondritis; (2) nasal chondritis; (3) respiratory tract chondritis; (4) non-erosive seronegative inflammatory polyarthritis; (5) ocular inflammation; (6) cochlear and/or vestibular dysfunction; (7) compatible histological features in a cartilage biopsy specimen. [2] We present a case of RP in a young female, which went undiagnosed for eight months and ultimately turned fatal immediately after diagnosis. A 30-year old female patient came to the Emergency Department with acute onset of breathlessness for two hours, accompanied by high-grade fever associated with swelling and redness of the left ear and watering of eyes, for past five days. The patient's past history was significant, with a similar episode of redness and swelling of the right ear, first appearing before eight months, with a waxing and waning course and subsiding before three months; leaving a deformity of the right ear. There was no history of joint pain or swelling of joints or any other skin lesions in the past. The patient was admitted and started on IV antibiotics after considering that her condition was cellulitis of the ear, and subsequently she was referred to the Dermatology Department to rule out drug reaction. We examined the patient thoroughly and investigated further. On examination, she was found to have high-grade fever (101° F.), wheezing, and dyspnea; swelling and redness of the conjunctiva and cornea, with watery discharge from both the eyes; inflamed, erythematous, and swollen left ear; deformity of both ears with sparing of ear lobes; deformity of nose (saddle nose) [Figure - 1],[Figure - 2] and partial deafness. No other skin, mucosal or nail lesions were observed. Superficial sensations (touch and temperature) were normal on examination. All routine investigations including hemoglobin, leucocyte count (total and differential), routine urine examination, and renal and liver function tests were within reference range; except ESR, which was 140 in the first hour. Mantoux test was negative; X-ray chest did not show any abnormality. Biopsy of the ear cartilage showed fragmentation of cartilage and replacement of cartilage by fibrous tissue, cartilage destruction with loss of basophilic staining and lymphocytic infiltrate was evident [Figure - 3]. Clinical findings and investigations, including biopsy, confirmed the diagnosis of relapsing polychondritis. The patient fulfilled six of the seven McAdams criteria [2] for the diagnosis (namely, bilateral auricular chondritis, nasal chondritis, respiratory tract chondritis, ocular inflammation, hearing loss, and compatible cartilage biopsy findings). The patient was prescribed oral prednisolone 40 mg per day, along with dapsone 100 mg daily. (G-6PD deficiency was ruled out). The patient did not come for the follow-up visit after discharge from the hospital. After about one month the patient again came to the Emergency Department with pain in her throat and hoarseness of voice. Unfortunately the patient collapsed within a few minutes. Relapsing polychondritis was first described in 1923 by Jaksch-Wartenhorst as polychondropathia, [3] and due to its episodic nature it was later on termed as 'relapsing polychondritis'. [4] RP is an uncommon, multisystem disease that can be life-threatening, debilitating, and difficult to diagnose. It is characterized by recurrent, potentially severe, and frightening episodes of inflammation of cartilaginous tissues. All types of cartilage may be involved, including the elastic cartilage of the ears and nose, the hyaline cartilage of peripheral joints, the fibrocartilage at the axial sites, and the cartilage in the tracheobronchial tree. RP can also inflame other proteoglycan-rich structures, such as the eye, heart, blood vessels, and inner ear. Systemic symptoms (like fever, lethargy, and weight loss) are common, and vasculitis, affecting skin or internal organs, may occur. The patients can present with a wide array of painful symptoms that often pose as major diagnostic dilemmas. As no specific tests are available for it, relapsing polychondritis must be diagnosed on clinical grounds. Pathogenetically, a linkage to HLADR4 and other autoimmune diseases has been noted. [1] In most patients, RP assumes a fluctuating but progressive course in which polycyclic bouts of inflammation eventually lead to permanent destruction of the involved structure. RP usually manifests between the third to fifth decade; average age of onset is 47 years. Male to female ratio of 1:3. This disease is usually seen in white persons; it has been rarely reported in other ethnic groups. [1] RP is considered as an autoimmune disease; with autoimmunity against type II collagen. Value of antibody titer in assessing the disease and its severity is debated. [5] Prognosis is variable and depends upon the organ involvement and response to treatment. A variety of anti-inflammatory and antineutrophilic agents, including corticosteroids, dapsone, NSAIDs, and methotrexate are reported to be useful. Of late successful results with infliximab and IL-1 receptor antagonist (anakinra) have been reported. [6] RP has been occasionally reported in Indian literature.[7],[8] Our case was a clinically typical case of relapsing polychondritis, but as mentioned earlier only ear and eye inflammation were present and she was misdiagnosed as a case of urticaria and angioedema, which was not reviewed again when tissue destruction was evident; leading to a delay in the targeted treatment. This might be the cause of the fatality in our case. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10019f2.jpg] [dv10019f1.jpg] [dv10019f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}