 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
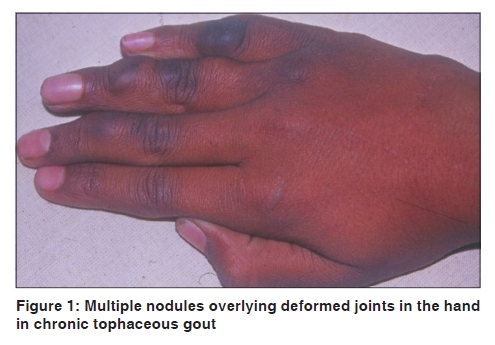
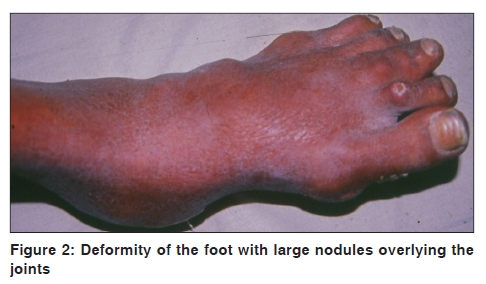
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 69-71 Letter to the Editor Chronic tophaceous gout with severe deforming arthritis Sujay Khandpur, Anil K.V. Minz, Vinod K. Sharma Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi India Code Number: dv10020 PMID: 20061741 DOI: 10.4103/0378-6323.58689 Sir, Gout is an inflammatory arthritis caused by cellular reaction to monosodium urate crystal deposition. Tophi are chalky, gritty accumulations of monosodium urate crystals that build up in soft tissue of an untreated gouty joint. Fortunately, advances in early diagnosis and treatment of gout have made such patients uncommon. We describe a dramatic clinical presentation of severe deforming arthritis due to chronic tophaceous gout. Such cases must be differentiated from other conditions manifesting as cutaneous nodules with crippling arthritis. A 40-year-old man presented with multiple nodules over bilateral hands, feet, elbows, knees and ankles since four years. The lesions were initially small and painless that gradually increased in size, some of which ulcerated and discharged white chalky material. His past history was remarkable for bilateral, asymmetric, large (wrists, elbows, knees, ankles) and small joint (interphalangeal joints of hands and metacarpophalangeal and interphalangeal joints of feet) pain with swelling and erythema of 11 years duration. He had taken only traditional medications without relief. There was no family history of gout, or personal history of hypertension, alcohol use, and high purine diet intake. His occupation did not involve chronic exposure to chemicals, heavy metals or aerosols. Dermatological examination revealed multiple, mobile, skin-to-yellowish colored, firm, dermal and subcutaneous nodules and large globose tumors, located on palms and dorsa of hands overlying interphalangeal joints, wrists, elbows, knees, ankles and interphalangeal joints of the feet [Figure - 1],[Figure - 2]. Some of the lesions ulcerated, discharging chalky material. The associated joints were deformed. His hematological and biochemical examination revealed anemia (Hb-5.6 gm/dl), raised serum uric acid (11.4 mg/dl, normal - 2-7.4 mg/dl), blood urea (110 mg/dl, normal - 10-50 mg/dl) and serum creatinine (2.0 mg/dl, normal - 0.5-1.8 mg/dl). Liver function test, urinalysis and serum electrolytes were within normal limits. Rheumatoid factor was negative. Radiographic evaluation of both hands showed soft-tissue swelling and periarticular erosions in the lower end of radius and interphalangeal joints with sclerotic margins and overhanging edges. Polarizing microscopy of the chalky material from the ulcerated nodules revealed negatively birefringent needle-shaped urate crystals. Skin biopsy from the finger nodule revealed upper dermal perivascular chronic inflammatory cell infiltrate with amorphous eosinophilic material deposited in the reticular dermis. A diagnosis of tophi with gout was made. He was started on ultra low dose allopurinol (100 mg/day) and NSAIDs, but left against medical advice before a detailed nephrology work-up could be initiated. Our patient was a case of chronic tophaceous gout (CTG) with severe disfiguring deformities and marked functional impairment. He presented for the first time to the dermatology OPD in view of multiple cutaneous nodules overlying joints and tendons on the hands, feet, elbows and knees. CTG usually manifests between 3-42 years (average 12 years) of initial untreated disease, due to accumulation of monosodium urate crystals around the joints (bursae, ligaments and tendons) especially the olecranon bursa, infrapatellar and Achilles' tendons and subcutaneous tissue on the extensors of extremities including wrists and hands. [1] They may also involve ear helix, nasal cartilage, eyelids, cornea, tricuspid and mitral valves. Some unusual presentations include erosive intraspinal and paravertebral lesions and carpal tunnel syndrome. [2] Cutaneous tophi appear as cream colored to yellowish nodules, are firm and mobile with overlying skin often being thin and red. Bullous tophi have also been reported. [3] Risk factors include chronic diuretic therapy, excessive alcohol consumption, chronic use of cyclosporine, postmenopausal age group and the inability to take hypouricemic drugs due to allergy or renal disease. Our patient had only taken traditional medicines for joint pains and did not resort to specific therapy for gout. The long-term neglect of the condition by the patient led to deterioration with tophi deposition in the joints. This condition has several mimickers which include histiocytic, rheumatological, infective, immunological and storage disorders. [4],[5] It must be differentiated from multicentric reticulohistiocytosis, which is characterized by deeply set, reddish-brown, non tender, small firm papules and nodules on the face ('coral beads' and vermicular lesions bordering the nostrils, ears and retroauricular region, eyelids), forearms, elbows and hands with progressive, bilateral, asymmetric, erosive polyarthropathy with interphalangeal joint predominance, minimal or absent periosteal reaction and mild osteoporosis compared to the severity of erosions. Histology shows histiocytes and multinucleate giant cells with 'ground glass' cytoplasm throughout the dermis. Rheumatoid nodule occurs in 25% cases of active RA in subcutaneous location, bursa and tendon sheaths over pressure sites such as olecranon process, extensors of forearms, hands and Achilles' tendons. Nodal generalized osteoarthritis occurs in menopausal women and shows multiple Heberden's nodules in distal interphalangeal joints and Bouchard's nodules in proximal interphalangeal joints with associated osteoarthritis. Pseudorheumatoid nodule is a juxta-articular form of nodular granuloma annulare with persistent nodules located in the small joints of the hands. Fibroblastic rheumatism is characterized by firm papules in the periungual area, hands and feet with associated polyarthritis. The nodules show dermal fibrosis interspersed with lympho-histiocytes. Tuberotendinous xanthomas present as multiple, grouped, yellowish brown nodules bilaterally on the trunk, knees, elbows, palms, soles, and dorsa of interphalangeal joints with raised triglyceride and cholesterol levels. Histopathology reveals many Touton giant cells and numerous foam cells in the dermis. Juvenile hyaline fibromatosis is an autosomal recessive mesenchymal dysplasia presenting as multiple subcutaneous tumors with flexion contractures of joints and radiolucent bone destruction. The lesions show amorphous hyaline material deposition in the extracellular spaces of the dermis and soft tissue. Other uncommon differential diagnosis include mucinous nodules overlying rheumatoid arthritic joints, accelerated rheumatoid nodulosis secondary to methotrexate therapy, synovial cysts over tendon sheaths and bursae, tenosynovial nodules associated with Human T lymphotropic virus-1, sarcoidosis, subcutaneous and tendinous nodules in scleroderma and rarely angioimmunoblastic t-cell lymphoma with arthritis. In our patient, the clinical features supplemented by characteristic laboratory and radiological findings helped in confirming the diagnosis. Complications of gout include renal involvement such as nephrolithiasis or acute and chronic gouty nephropathy. [1] In our patient, renal function was deranged although a detailed evaluation could not be undertaken. Treatment of CTG includes diet modification, medical and surgical therapy. [1] Medical treatment includes NSAIDs, hypouricemic drugs like allopurinol and uricosuric drugs like probenecid and sulfinpyrazone. Surgery is usually avoided unless tophi are in a critical location, drain chronically or there is intractable joint pain, loss of motion and massive joint destruction. The conventional enucleating procedure may lead to complications such as skin necrosis, tendon or joint exposure. A 'shaver technique' for deformity management of CTG has been described. [6] References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10020f1.jpg] [dv10020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}