 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
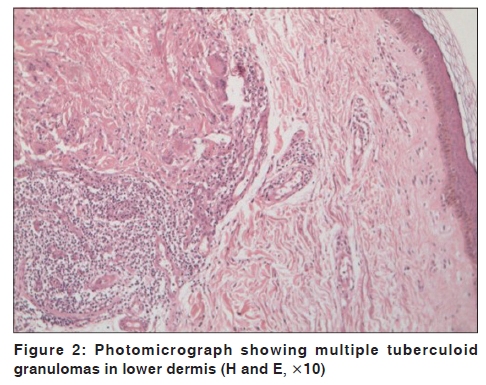
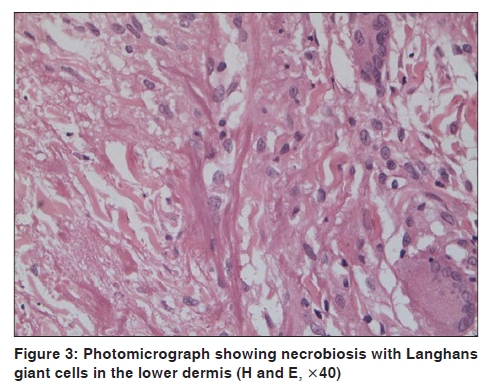
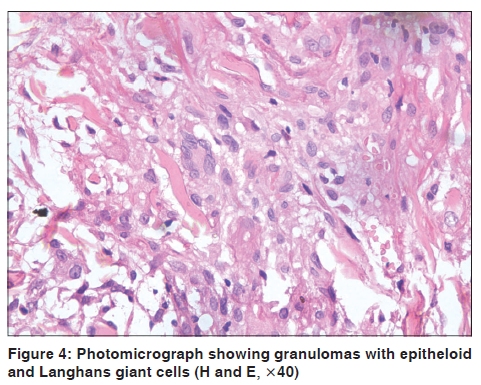
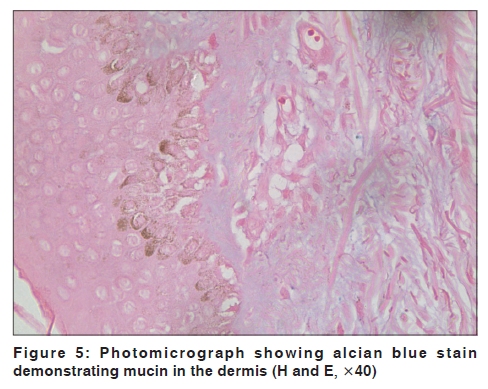
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 73-75 Letter to the Editor Generalized granuloma annulare with tuberculoid granulomas: A rare histopathological variant Sekar C. Shanmuga, Reena Rai, A. Laila, S. Shanthakumari1, V. Sandhya1 Departments of Dermatology and, 1Pathology, PSG Hospitals, Coimbatore, India Code Number: dv10022 PMID: 20061743 DOI: 10.4103/0378-6323.58691 Sir, Colcott Fox first described granuloma annulare (GA) in 1895 [1] and in 1902 Radcliffe-Crocker labeled it as Granuloma annulare. [2] Granuloma Annulare is a benign granulomatous disease of unknown etiology characterized by multiple erythematous and annular plaques with histopathological features of necrobiosis and palisading granulomas. The clinical variants include localized, generalized, perforating and subcutaneous types. Common histological variants are palisading and interstitial granulomas, however, tuberculoid or sarcoidal granulomas occur rarely. [3] We report a case of generalized granuloma annulare with tuberculoid granulomas. A 65-year-old female presented with multiple well defined annular erythematous plaques on both hands and lower legs of two years duration [Figure - 1]. On examination, the sensations over the plaques were intact and there were no palpable nerves. A clinical differential diagnosis of granuloma annulare and Hansen's disease were made. Histopathology revealed a normal epidermis with mid to deep dermis showing perivascular and periadenexal collection of lymhocytes. Multiple ill defined granulomas composed of epitheloid cells and Langhans giant cells [Figure - 2],[Figure - 3],[Figure - 4] with fibrin and altered collagen were also found. Alcian blue stain showed mucin deposits in the dermis [Figure - 5]. Fite stain was negative. With these histopathological findings a diagnosis of tuberculoid variant of generalized granuloma annulare was made. Granuloma annulare is a granulomatous disorder, which is more common in females. The age of onset is usually less than 30 years. Several precipitating factors have been proposed, which include sun exposure, insect bites, viral infections, thyroiditis, tuberculin skin tests and trauma. [1] Granuloma annulare (GA) has varying clinical presentations that include localized, generalized, subcutaneous, and perforating forms. A generalized form of granuloma annulare can occur in up to 15% of patients, and is characterized by multiple, asymptomatic, erythematous or skin-colored plaques located primarily on neck, trunk and extensor surfaces of extremities. [4] Generalized granuloma annulare is characterized by a later onset, poorer response to therapy and an increased prevalence of the HLA-Bw35 allele. [4] Alterations in the lipid profile (hypercholesterolemia, hypertriglyceridemia, or both) were found to occur in 45% of patients with generalized granuloma annulare. [4] Generalized granuloma annulare may represent a paraneoplastic phenomenon in patients with lymphoma or other malignant conditions. Granuloma annulare is characterized by three different histolopathological patterns. The most common is the interstitial pattern, in which histiocytes infiltrate between collagen fibers and minimal degenerated collagen is noted. The second is the classic pattern, in which there are palisaded granulomas in the dermis. Degenerated collagen fibers and mucin form the center of the granulomas are surrounded by histiocytes and lymphocytes. The last pattern is composed of epithelioid histiocytes and can resemble sarcoidosis or tuberculosis as seen in our case. Tuberculoid granulomas are characterized by focal collection of lymphocytes, epitheloid cells and Langhans giant cells with or without central necrosis. They are commonly seen in cutaneous tuberculosis, tuberculoid leprosy and foreign body granulomas. Friedman et al., compared the histopathological patterns of localized and generalized granuloma annulare and found that the interstitial pattern was more in localized diseases and the prevalence of palisaded pattern was equal among both clinical types. No data is available regarding the prevalence of tuberculoid granulomas in granuloma annulare. It is considered one of the rarer patterns. We report this case because the association of disseminated granuloma annulare with tuberculoid granulomas has never been reported.[5] References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10022f4.jpg] [dv10022f2.jpg] [dv10022f5.jpg] [dv10022f3.jpg] [dv10022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}