 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
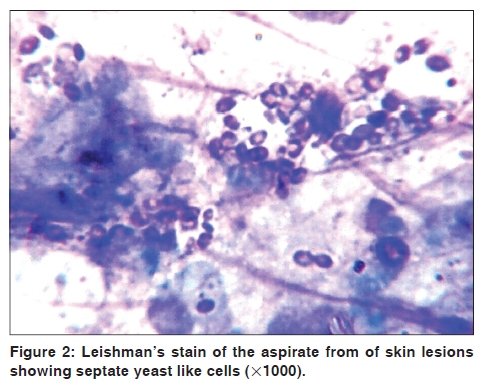
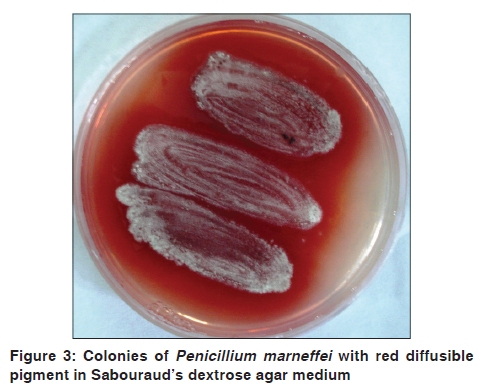
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 75-76 Letter to the Editor Penicillium marneffei infection in Assam Lahari Saikia, Reema Nath, J. Mahanta1 Department of Microbiology, Assam Medical College, Dibrugarh - 786 002, Code Number: dv10023 PMID: 20061744 DOI: 10.4103/0378-6323.58692 Sir, Penicillium marneffei infection in human immunodeficiency virus (HIV) infected patients is being increasingly observed in Southeast Asia since 1988, and is considered as an AIDS defining illness. [1],[2] In India, although the maximum cases of penicillosis have been reported from Manipur, yet cases in the bordering states like Assam and Nagaland are very rare, although the environmental conditions are similar. We describe here the occurrence of Penicillium marneffei infection in a HIV-infected female patient from Assam. A 27-year-old, female, HIV seropositive patient from Assam, presented with high-grade fever, cough, weight loss, diarrhea, and generalized papular skin rash of three months duration [Figure - 1]. She gave no history of moving out of Assam. Her skin lesions were smooth, dome-shaped, umbilicated, and varying in size, from 1-3 mm. The patient had oral thrush and symptoms of esophageal candidiasis along with ulcerative vaginal lesions. She was also under antitubercular therapy for the last two months. Differential diagnosis of disseminated penicillosis and molluscum contagiosum with HIV infection was considered on the basis of the skin lesions. Her hemoglobin was 9.4 gm/dl, leukocyte count 8900/ μl, and erythrocyte sedimentation rate was 135 mm, at the end of the first hour. Her absolute CD41 t -cell count was 37 cells/μl of blood. Leishman's stain of the aspirate from the skin lesions showed intracellular and extracellular septate yeast-like cells [Figure - 2]. Culture of the aspirated fluid in Sabouraud's dextrose agar (SDA) showed flat, glabrous, moist, radially folded colonies, with diffusible red pigment after five days of incubation at 25°C [Figure - 3]. Microscopic examination revealed septate hyphae with lateral and terminal conidiophores and chains of ovate conidia, characteristic of the Penicillium species. A culture at 37°C showed moist, flat, brownish white colonies of septate yeast-like cells after five days of incubation. The patient was advised to stay in hospital, but left the hospital against medical advice . Penicillium marneffei is a dimorphic fungus, which causes fatal infection in HIV-infected patients, usually when the CD4 1 t -cell count goes below 50 cells/ μl. Most often, they present with fever, weight loss, anorexia, and papular skin lesions, resembling molluscum contagiosum. [3],[4] A tropical climate with high humidity and rainfall is favorable for fungal growth. Although all the states in the North Eastern region have a similar climate, yet penicillosis is rare in all other states except Manipur. Now the clinicians of Manipur are aware of such an infection among AIDS patients. Varghese et al., reported, for the first time, a case of disseminated Penicillium marneffei infection from Assam. [5] Report of this case indicates an inroad of penicillosis to Assam, which may be an added misery for the AIDS patients of the state. Therefore, clinicians of the state need to maintain a high index of suspicion for making an early diagnosis, for treatment of such rare cases, in this state. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10023f1.jpg] [dv10023f2.jpg] [dv10023f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}