 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
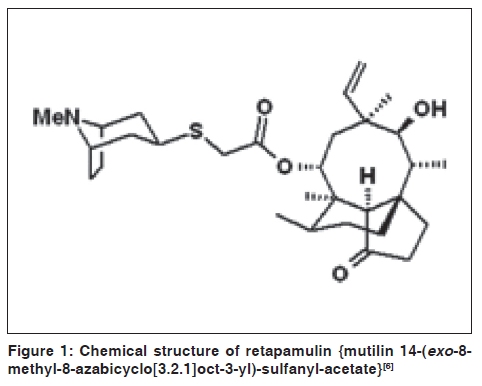
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 77-79 Focus Retapamulin: A novel topical antibiotic H. Nagabushan Department of Pharmacology, K.S. Hegde Medical Academy, Mangalore, Karnataka, India Code Number: dv10024 PMID: 20061745 DOI: 10.4103/0378-6323.58693 Introduction Skin infections are a common reason for patients to seek attention from dermatologists. The most common bacteria found in skin and soft tissue infections (SSTI) include the gram-positive organisms Staphylococcus aureus (55.2%), β- hemolytic Streptococci (5.0%), and Coagulase- negative Staphylococci (4.9%). Most of these bacteria causing SSTI have become resistant to the leading topical antimicrobials used in clinical practice. Antibiotics with a novel mechanism of action are needed to address the rising resistance to established classes of both systemic and topical agents. Resistance has already developed to two of the most commonly used topical antibiotics, fusidic acid and mupirocin. [1] Retapamulin, a novel topical antibacterial agent, will probably replace the use of mupirocin and fusidic acid. [2] It was approved by FDA, in 2007, for topical treatment of impetigo. [3] European Medicines Agency approved this drug also for infected wounds caused by S. pyogenes and methicillin susceptible S. aureus. [4] Synthesis Retapamulin is a derivative of the naturally occurring pleuromutilin, produced by Pleurotus mutilins (now called Clitopilus scyphoides), an edible mushroom. [5] Pleuromutilin was discovered in 1951, but it was not until the early 1970s that its potential for use as an antimicrobial was more fully recognized. Other agents in this class (tiamulin and valnemulin) have been developed as veterinary antibiotics. These drugs have a common tricyclic mutilin core, a C21 keto group, essential for antimicrobial activity and various substituents at its C14, most of which are extensions of diverse chemical nature. Retapamulin is a C14-sulfanyl-acetate derivative of pleuromutilin [Figure - 1]. Mechanism of Action The pleuromutilin class has a unique mode of action which involves inhibition of bacterial protein synthesis at the level of bacterial 50s ribosome. [1] It binds to domain V of 23s rRNA, inhibits ribosomal peptidyl transferase activity and partially inhibits the binding of the initiator tRNA substrate to the ribosomal P-site. [7] The ribosomal binding site for pleuromutilin overlaps with that for chloramphenicol and puromycin, hence both drugs compete with retapamulin for the binding site. [8] Antimicrobial spectrum Retapamulin is effective against gram-positive and some gram-negative organisms. It includes Streptococcus pyogenes, Streptococcus agalactiae, b-hemolytic streptococci, Streptococci viridans, Staphylococcus aureus, Coagulase-negative staphylococci, Propionibacterium spp (including P acnes), Prevotella spp, Porphyromonas spp, Fusobacterium spp, Bacteroides and Clostridium. It is a bacteriostatic drug, but may be bactericidal at high concentration. The minimum bactericidal concentration (MBC) is 1000 times higher than the minimum inhibitory concentration (MIC).The MIC against S. aureus is between 0.03 and 0.25 mcg/ml and for S. pyogenes it is between 0.008 and 0.03 mcg/ml. [9] It has substantial post antibiotic effect (PAE) against S. aureus and S. pyogenes, which may contribute to the efficacy observed after twice daily application of 1% ointment. [10] However, retapamulin showed minimal or no activity against enterococci and gram-negative bacilli. It is active against B. fragilis but less active against other members of the B. fragilis group, especially B. thetaiotaomicron. It is as potent as Co-amoxiclav, imipenem, metronidazole and clindamycin against Prevotella spp, Porphyromonas spp and Fusobacterium spp. It is also more active than clindamycin, metronidazole and ceftriaxone against anerobic gram- positive cocci. [11] Most importantly, it maintains its activity against organisms that are resistant to a number of antimicrobials including methicillin, erythromycin, fusidic acid, mupirocin, azithromycin and levofloxacin. Pharmacokinetics Bioavailability is low. Hence systemic exposure is minimal following topical application to intact or abraded skin. It is 94% protein bound and metabolized in liver by monooxygenation and N-demethylation to numerous metabolites. The main enzyme responsible for metabolism in liver microsome is CYP3A4. Side effects The most common adverse effect is pruritus at the application site. [12] Others are blisters, burning, redness, swelling, headache, diarrhea, eczema and oozing at the site where the ointment is applied. Retapamulin is classified as pregnancy category B; however, there have been no adequate human studies in this population group. Drug resistance Retapamulin has demonstrated excellent activity in vitro against S. aureus, irrespective of their level of resistance to other antimicrobials. [13] One study has shown that bacterial resistance in vitro is through two mechanisms: Mutation in protein L3 close to the peptidyl transferase center and the development of drug efflux mechanisms. [14] Mutation in L3 is a multi-step process which appears to be slow to emerge. Evidences from multiple-step and single-step studies also suggest that retapamulin has a low potential to select for resistant mutants in S. pyogenes and S. aureus. Retapamulin had the lowest rate of spontaneous mutations by single step passaging and the lowest parent and selected mutant MICs by multi step passaging among all drugs tested for all S. aureus strains and three S. pyogenes strains which yielded resistant clones. [15] Another study showed a stepwise reduction in pleuromutilin susceptibility occurring concurrently with stepwise acquisition of mutations in rplC. [16] A potential clinical threat of cross-resistance in the antibiotics that targets the ribosomal peptidyl transferase center (PTC) is the multidrug resistance phenotype mediated by the cfr rRNA methyltransferase. This gene encodes a methyltransferase that modifies the PTC nucleotide A2503, and is responsible for resistance to phenicols, lincosamides, oxazolidinones, pleuromutilins, and streptogramin antibiotics. [17] Dosage and administration A thin layer of retapamulin should be applied to the affected area (up to 100 cm 2 in total area in adults or 2% total body surface area in pediatric patients aged nine months or older) twice daily for five days. The treated area may be covered with a sterile bandage or gauze dressing if desired. Drug interactions Drug interactions are less due to low systemic exposure following topical application. Dosage adjustments are unnecessary when co-administered with CYP3A4 inhibitors such as ketoconazole. Indications It is used in adults and children over nine months of age for topical treatment of impetigo and infected wounds caused by S. pyogenes and methicillin susceptible S. aureus (MSSA). [3],[4] Conclusions Retapamulin, a novel pleuromutilin derivative, could probably provide a valuable therapeutic option for the management of skin and soft tissue infections caused by S. pyogenes and S. aureus resistant to the most commonly used topical antibiotics. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10024f1.jpg] |
| |||||||||

{kind=link}