 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
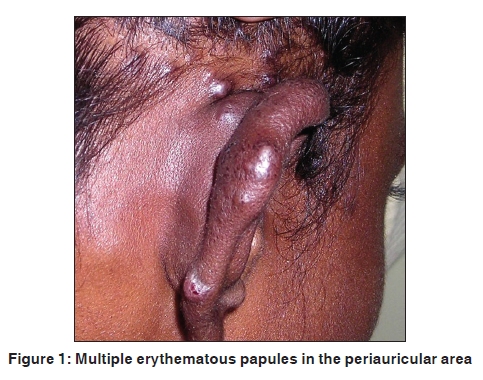
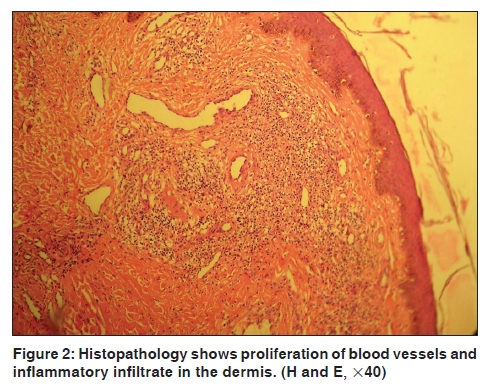
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 83-84 Quiz Multiple erythematous papules on the pinna Veeranna Shastry, Vijaya1 Department of Dermatology, Venereology and Leprosy, 1Pathology, J.S.S Medical College and Hospital, Mysore, Karnataka - 570 004, India Code Number: dv10026 PMID: 20061747 DOI: 10.4103/0378-6323.58696 A 19-year-old male presented with itchy lesions over the right periauricular area since four months. It was gradual in onset. There was history of occasional bleeding from the lesions and each individual lesion persisted indefinitely. There was no history of trauma, pain or any ear symptom. On examination there were multiple, grouped, erythematous papules measuring 4-8 mm, situated on the right pinna, supra and retroauricular area [Figure - 1]. There was no regional lymphadenopathy. Hemogram and urinalysis was normal. Histopathological features from one of the papule are shown in [Figure - 2] and [Figure - 3].
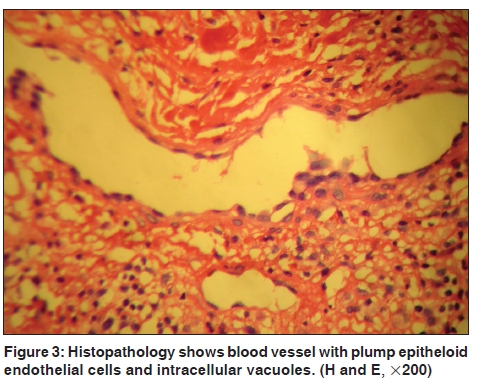
What is your Diagnosis? Histopathology showed mild acanthosis and proliferation of blood vessels in dermis [Figure - 2]. The vessels were lined by plump epitheloid endothelial cells [Figure - 3]. Intracytoplasmic vacuoles were seen in some of the endothelial cells. There was nodular proliferation of inflammatory cells in the dermis consisting of lymphocytes, histiocytes and eosinophils. Lesions were treated with topical steroids for three weeks; there was no improvement, treatment was changed to topical imiquimod and the patient lost to follow-up. Discussio Angiolymphoid hyperplasia with eosinophilia (ALHE) also known as epitheloid hemangioma is an uncommon distinct clinical and pathologic entity that demonstrates proliferation of endothelial cells associated with varying degrees of lymphocytic, histiocytic, and eosinophilic infiltration. [1] The exact cause of ALHE is unknown; however, there have been several proposed theories, including environmental factors, such as insect bites or parasites, trauma, hyper estrogen states, and immunologic mechanisms. Some authors have also suggested that it may be secondary to an inflammatory vascular reaction, a neoplastic process, or a neovascular formation from preexisting blood vessels. [2] Cases in association with trauma, anomalous dilatation of arteries, AV malformation and oral contraceptives [3] have been described. It is more common in young adults in the head and neck region, particularly, around the ear. It presents as multiple, grouped, erythematous papules or nodules. Occasionally, deeper extension and large subcutaneous lesions can occur. Less frequently, lesions arise from the trunk and extremity, oral mucosa and bone. Peripheral eosinophilia is seen in 20% of the cases, the course is chronic and spontaneous regression is seen in majority of the cases. [4] Histopathology shows proliferation of small to medium sized blood vessels often showing lobular architecture. These vessels are lined by plump, epitheloid endothelial cells which project into the lumina. The nucleus of these cells is ovoid without atypia. Some of these cells often show intracytoplasmic vacuoles. [5] The cellular infiltrate around the vessels is composed of lymphocytes and eosinophils. Older lesions show fibrosis. The clinical differential diagnoses include pyogenic granuloma, Kimura's disease and Kaposi's sarcoma. Histopathologically, it has to be differentiated from angiosarcoma, insect bite reaction, pyogenic granuloma and Kimura's disease. [5] Although ALHE is considered a benign disease, it can be resistant to multiple therapies, and can become disfiguring to the patient. Various therapeutic modalities like, excision, electrosurgery, cryo surgery, laser ablation, topical and intralesional steroids, Interferon α 2b, oral retinoids and topical imiquimod have been used to treat this condition. [3] References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10026f3.jpg] [dv10026f2.jpg] [dv10026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}