 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
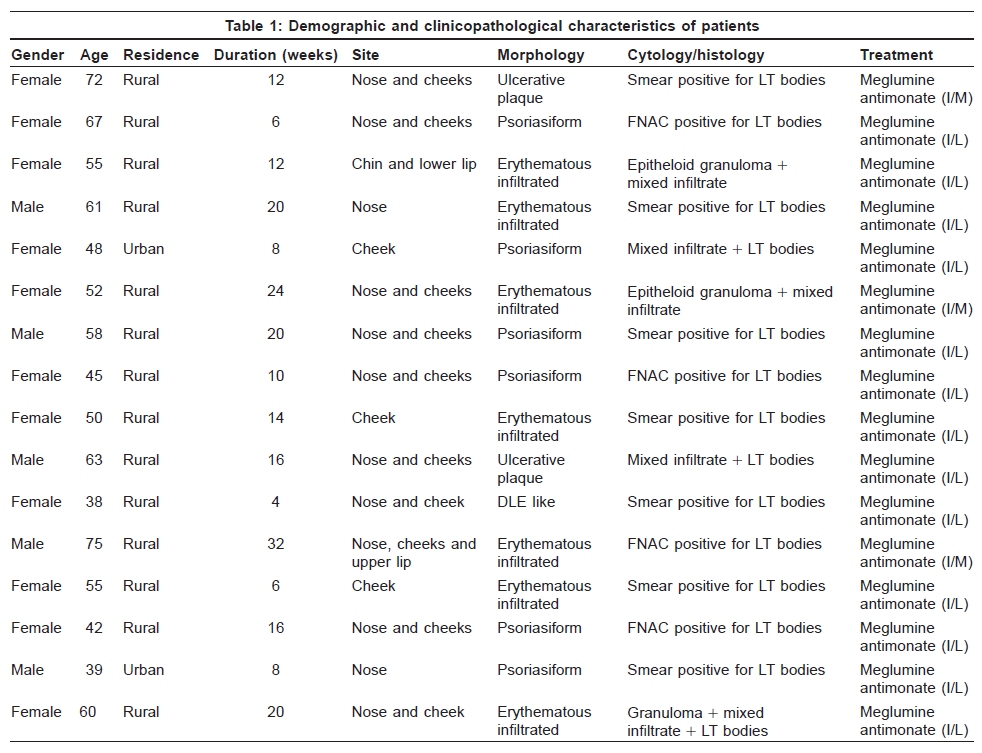
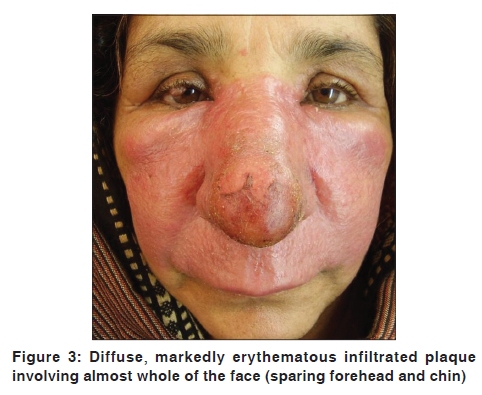
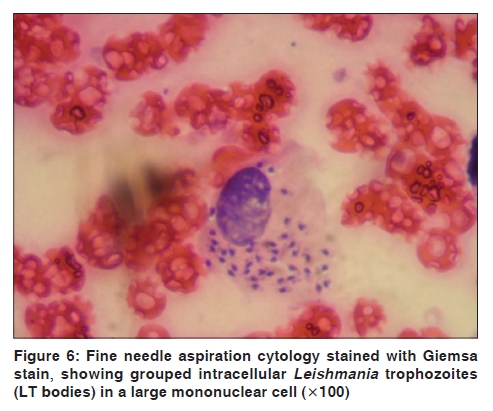
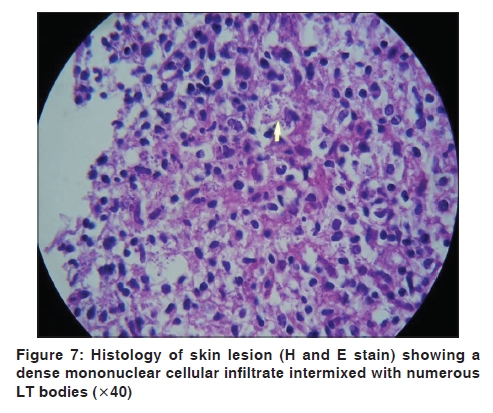
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 85 Net Study Lupoid cutaneous leishmaniasis: A report of 16 cases Arfan Ul Bari, Naeem Raza1 Department of Dermatology, Combined Military Hospital, Peshawar, 1PAF Hospital, Faisal, Karachi-Pakistan Code Number: dv10027 PMID: 20061750 DOI: 10.4103/0378-6323.58698 Abstract Background: Lupoid cutaneous leishmaniasis (CL) is known as the chronic form of CL. However, keeping its clinical presentation in view, there is a need to revisit this form of disease. Aims: To redefine/describe lupoid CL in view of clinical features. Methods: It was a case series seen in Muzaffarabad (Pakistan) from Jan 2006 to May 2008. All patients clinically suggestive and consistent with laboratory diagnosis of CL were registered. Patients of all age groups and either sex having cutaneous lesions resembling lupus vulgaris or lupus erythematosus on the face or elsewhere were included in the study. Those having chronic fluctuating/relapsing course or scarring within the lesions were also included. Various demographic features of the patients and clinical patterns were recorded. Descriptive statistics were used for analysis. Results: Of 254 registered patients of CL, 16 (6.3%) were diagnosed as lupoid CL. None of the patients had scarred lesions. Age ranged from 38 to 75 (55 + 15.11) years and duration of lesions varied from 4 to 32 (14.25 + 07.59) weeks. All patients had lesions over the face. Thirteen (81.25%) had a large solitary plaque extending over the nose and a large part of the cheeks and three (18.75%) had multiple lesions. Lesions were central/nasal in two (12.5%), unilateral/asymmetrical in four (25%) and bilateral/symmetrical in 10 (62.5%). Morphological patterns included erythematous/infiltrated (7), psoriasiform (6), ulcerated/crusted (2) and Discoid lupus erythematosus (DLE)[G1] like (1). Conclusion: Lupoid CL is not strictly a chronic form of disease, which presents on the face from the very onset and shows no scarring or recurrence. Keywords: Chronic cutaneous leishmaniasis, Cutaneous leishmaniasis, Lupoid cutaneous leishmaniasis Introduction The diverse clinical spectrum of cutaneous leishmaniasis (CL) is dependent on a number of factors, such as the type and duration of clinical lesion, strain of organism, geographic location, parasitic load, disease reservoir and host immunocompetence, etc. [1],[2] During the usual course of the disease, there is an evolution of lesions as they progress from a papule/nodule to an infiltrated, indurated, crusted plaque/nodule. The lesion then usually breaks open, after a varying period of 3-4 months, into a well-circumscribed ulcer, which heals slowly over a period of 3-12 months. Occasionally, the healing does not take place and the lesion may then persist as a chronic yellow-brown firm nodule. [1],[2],[3],[4] Opinion has varied for the definition of chronic lesions, with different criteria (6 months to 2 years) being quoted by different authors. [2] Lupoid CL is a particular form of CL with characteristic spreading of the initial lesion leading to an erythematous, infiltrated plaque. Sometimes, brown-red or brown-yellow papules appear. Subsequently, they coalesce and form a plaque closely resembling Lupus vulgaris (LV), even to the formation of apple-jelly nodules. Although not as destructive as LV, lupoid CL may persist and spread for many years. [4],[5] Leishmaniasis recidivans (LR), although frequently used for lupoid CL, is a distinctive form of chronic CL that is usually a complication of Leishmania tropica in the old world and less commonly Leishmania braziliensis in South America. [6] LR refers to the development of new lesions in the center or periphery of a healed acute lesion of CL. Clinically, there is a central scar in which central or peripheral infiltrated papules and crusted inflammatory lesions develop that expands slowly, assuming a circular or arciform configuration. The lesions tend to resist treatment and become chronic. Chronicity of the (CL) lesion is thought to be the result of a peculiar host reaction in which cellular immunity fails to sterilize the lesion, despite the presence of exaggerated hypersensitivity. [4],[5],[6],[7],[8] Lupoid CL has also been described in the literature as being a chronic form that has a relapsing course and resists treatment like LR. The present study is aimed to describe the clinical features of lupoid CL in context with clinical features of chronic CL described in the medical literature. Because lupoid CL and LR have been frequently used interchangeably for the chronic form of CL, this is also an attempt to differentiate these two entities. Methods The study was conducted at the dermatology outpatient department of CMH, Muzaffarabad, over a period of 29 months from January 2006 to May 2008. All patients belonging to the Muzaffarabad district and its surrounding areas, irrespective of their age and sex and duration of disease, diagnosed clinically and substantiated with laboratory as cases of CL were initially registered. Patients of CL having non-circumscribed, diffuse erythematous/psoriasiform/infiltrated lesions (resembling lupus vulgaris [LV] or lupus erythematosus [LE]) on the face or elsewhere were included in the study and those who were partially treated for the disease earlier were excluded. Patients with lesions not clinically resembling lupoid but having history of fluctuating course, scarring within the lesions or reactivation of previously healed/partially healed lesions were also included. Diagnosis was based on history of origin of the patient (endemic areas) and clinical characteristics of lesions (painless, non-itchy, slowly evolving nodule, plaque or ulcer on exposed areas of the body not responding to conventional antibiotics). Clinical diagnosis was then confirmed by slit skin smear (SSS) or fine needle aspiration cytology smears. Skin biopsy was performed in selected cases (where cytology did not confirm diagnosis). All the patients finally included in the study had either positive SSSs or positive histology for Leishmania parasite. A standard protocol was followed for each patient. Detailed demographic features, duration of disease, number and site of lesions, morphological patterns of disease and treatment modalities employed were recorded in all cases. Patients were explained about the study in the language they understood and informed consent was obtained from all patients. Patients who agreed to indoor treatment were treated with daily intramuscular injections of meglumine antimonite (20 mg/kg) and those who could not afford hospitalization were treated with weekly local infiltration of all parts of the lesions with meglumine antimonate. Treatment was continued till clinical healing of the lesions. After treatment, patients were advised for follow-up monthly for 6 months and then bimonthly during a further 6 months to look for any recurrence. Computer program SPSS version 10 was used to manage and analyze data. Descriptive statistics (frequencies and percentages) were obtained for the variables where applicable. Mean and standard deviation were calculated for continuous variables. The study was approved by the scientific and ethics committee of the hospital. Results During the 29-month period, 254 patients were registered as cases of CL. Of these, 16 (6.3%) were found to have lupoid leishmaniasis. None of the patient had scarred lesions. The male to female ratio for lupoid cases was 1:2.2. Age ranged from 38 to 75 years (median = 55) and duration of lesions varied from 4 weeks to 32 weeks (median = 13). All the 16 patients had lesions over the face without involving any other part of the body. Thirteen patients (81.25%) had a large solitary plaque extending over the nose and a large part of the cheeks. Three (18.75%) had multiple lesions on the face. Lesions were central/nasal in two (12.5%), unilateral/asymmetrical in four (25%) and bilateral/symmetrical (large solitary lesion involving symmetrically both sides of the face and nose) in 10 (62.5%) patients. All of them belonged to known endemic areas and predominantly (87.5%) from a rural background. Demographic features of the patients are given in more detail in [Table - 1]. Four different morphological patterns of lupoid CL were observed, which included erythematous/infiltrated (7), psoriasiform (6), ulcerated/crusted (2) and DLE like (1). All the patients were satisfactorily treated with meglumine antimonate (13 with weekly intralesional injections for 8-16 weeks and three patients were given daily intramuscular injections for 14-20 days). Twelve of 16 patients completed 1 year follow-up and the remaining four are being followed-up (two of them have been followed-up for 8 months and two have completed 4 months so far). None of the patients showed any signs of recurrence/relapse of the disease. Some morphological patterns are shown in [Figure - 1] (crusted), [Figure - 2] and [Figure - 3] (diffuse, infiltrated and scaly), [Figure - 4] (psoriasiform) and [Figure - 5] (DLE like). Photomicrographs of the cytology smear and histopathology are represented in [Figure - 6] and [Figure - 7]. Discussion Lupoid CL has long been described as a unique form of CL characterized by unusual clinical features and a chronic relapsing course. In the medical dictionary, [9] the term "Lupoid" means resembling lupus and "lupus" means any of various skin conditions characterized by ulcerative lesions that spread over the body. Morphologically, it mimics lesions of LV or LE. There is no consensus for the definition of chronic lesions of CL as various authors quote different criteria for chronicity. [2] Due to the wide variety of clinical pictures, several terms have been used in the literature for lupoid CL. LR, also termed as relapsing leishmaniasis, has frequently been used for lupoid CL. [7],[8],[9] Clinically, lupoid CL may be similar to LE or LV, but histologically (being a granulomatous disorder), it looks more like LV, which is thus the most important differential diagnostic consideration and all patients with granulomatous facial lesions from endemic areas or with a positive travel history should be suspected of having CL. [7],[10],[11],[12] Although lupoid CL has previously been described in the literature frequently, its variable morphological spectrum was not emphasized before and most of the times the term was loosely applied for any form of chronic or relapsing CL. [13],[14],[15],[16],[17] The frequency of lupoid CL in our study reveals that it is no more a rare variant of CL as previously thought in our part of the world. However, it remains to be determined if this form of the disease is an altered immune response of the patient or a different organism is involved in its causation. Although lupoid CL has been reported in children, [18] none of the patients in the study were below the age of 38. Lupoid lesions have been described to occur on various body regions, [11] but in our patients, disease was restricted only to the face and the most common presentation was a large psoriasiform and erythematous infiltrated plaque. Probably, laxity of facial tissue and rich vascularization had been a contributing factor in producing large diffuse erythematous plaques of LL on the face. [12] Clinical course of lupoid leishmaniasis is thought to be related to changes in cell-mediated immunity that lead to localized or diffuse lesions. The described possible underlying pathogenetic mechanism is an altered balance between TH1 and TH2 cells, with consequent production of IL-4. This altered immune host response is assumed to have contribution in high susceptibility to parasitic infections and to the unusual clinical presentation. Because TH1-type cellular immune responses play a critical role in protection against Leishmania parasite, whereas TH2-type cell activation is thought to result in progressive disease, it is this TH2-type response that is believed to be involved in chronicity and persistence of lesions and delayed or unsatisfactory treatment response in cases of chronic (lupoid/recidevans) cases of CL. [7],[19],[20],[21],[22] However, considering the non-chronic course and excellent response to treatment in all cases of Lupoid CL in our study, the postulated cellular immune mechanism discussed above seems unlikely to operate fully here and the possible role of a new emergent causative species or any mutation in the already prevalent strain causing chronic lesions in the region (L. tropica) [23] cannot be ruled out. This was a limitation of the study that due to non-availability of advanced molecular diagnostic laboratory methods like polymerase chain reaction, we were not able to characterize the zymodeme type of parasite in the region. This study also has revealed a few clinical observations that are different from other forms of chronic CL. Although minimum duration for the lesions of cutaneous leshmaniasis to be labeled as chronic form is 6 months, [2] 14 of the 16 (87.5%) patients had lupoid lesions of less than 6 months duration. All the patients responded very well to intralesional or intramuscular meglumine antimonate without any adverse effects or residual scars and none of the patients relapsed or reactivated during follow-up. The study also highlighted that these cases can easily and effectively be treated with weekly intralesional injections of an antimonial compound, which is a much more cost-effective, safe and convenient way of treatment in most cases of lupoid CL as against systemic antimonial compounds. [24],[25] Considering these observations, we suggest that lupoid CL should be treated as a different entity than other chronic forms of CL because the hallmarks of chronic CL (chronicity and relapsing, scarring and reactivating course) are clearly lacking in all our patients. Morphologically, the term lupoid CL may be restricted to cases resembling DLE, Systemic lupus erythematosus (SLE)[G2] or non-scarring/non-relapsing cases of LV. Chronic relapsing/scarring or persistent, non-responding cases should be categorized as LR, leishmaniasis cicatrix or chronic scarring CL. These unique clinical characteristics and morphological spectrum of lupoid cases described here suggest that lupoid CL should be revisited and redefined. Conclusion Lupoid leishmaniasis is not a rare entity in the Azad Kashmir region of Pakistan. Clinically, it presents on the face as lupoid lesions from the very onset, responds favorably to standard treatment and heals without scarring or relapse/reactivation. It does not strictly represent a chronic form of disease and may be differentiated from LR (chronic scarring form of CL). References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10027f5.jpg] [dv10027f4.jpg] [dv10027t1.jpg] [dv10027f2.jpg] [dv10027f6.jpg] [dv10027f1.jpg] [dv10027f3.jpg] [dv10027f7.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}