 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
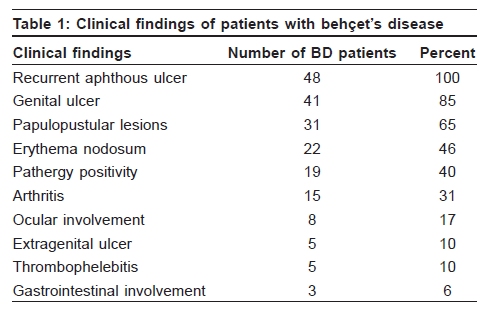
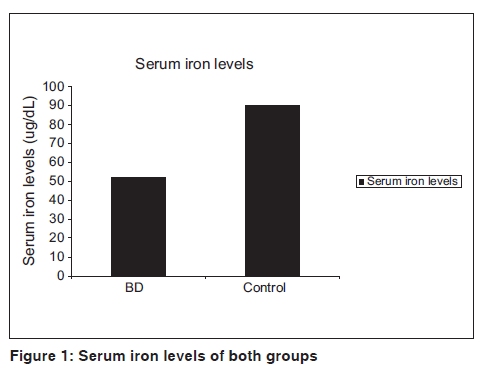
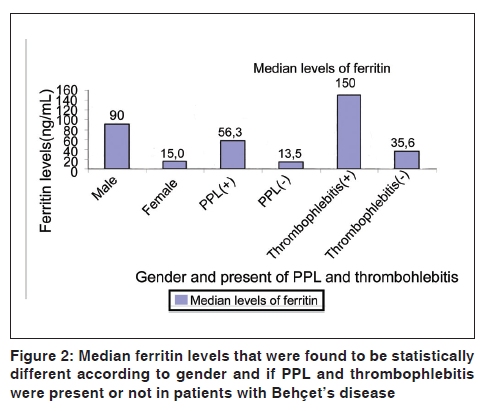
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 85 Net letter Serum iron and ferritin levels in Behçet's disease Müzeyyen Gönül, Ülker Gül, Seray Külcü Çakmak, Seçil Soylu, Arzu Kılıç Ankara Numune Education and Research Hospital, 2nd Dermatology Clinic, Ankara, Turkey Code Number: dv10029 PMID: 20061748 DOI: 10.4103/0378-6323.58700 Sir, Behçet's disease (BD) is a multisystem inflammatory disorder of unknown cause. Recently, it has been reported that oxidative stress and endothelial dysfunction may cause the vascular injury in BD. [1] Iron is involved in the antioxidative system and large amounts of iron are sequestered by ferritin. There are few reports investigating serum ferritin levels in BD. [2] We investigated the levels of serum ferritin, iron and iron binding capacity (IBC) in BD patients. The study consisted of 48 BD patients who were diagnosed according to the criteria of the International Study Group for BD and 49 sex- and age-matched individuals as the healthy control group. Exclusion criteria were disorders effecting the ferritin levels and use of iron preperations. The duration of the disorder, current and previous findings of BD patients and serum iron, IBC and ferritin levels of the patients and controls were obtained retrospectively. Disease activity was determined by the presence of at least one symptom within the last month at the time of blood sampling. Data were compared statistically by the Mann-Whitney U test and Spearman correlation test. Twenty-five women and 23 men with BD were enrolled in the study. Mean age was 37.82 ± 10.87 years. Median duration of disorder was 4 years (range 0.1- 26 years). The clinical features of BD patients are represented in [Table - 1]. Median iron levels were 52 mg/dl in the BD group and 90 μg/ dl in the control group. Serum iron levels were statistically lower in BD patients than those in controls (P < 0.009) [Figure - 1]. The mean IBC level and the median ferritin level were not significantly different in both the groups (262.4 ± 50.8 ug/dl and 42.10 ng/ml in BD patients, 266.4 ± 46.2 ug/dl and 42.4 ng/ml in the control, respectively). Ferritin levels did not show a statistical difference according to the activity and duration of BD. The median ferritin level was significantly lower in females (14.9 ng/ml) than in males (90 ng/ml) (P < 0.001) [Figure - 2]. However, there was no difference in the iron and ferritin levels according to age, sex and duration of the disease ( P > 0.05). Ferritin levels were significantly higher in patients with papulopustular lesions(PPL) and thrombophlebitis ( P = 0.022) [Figure - 2]. Although the pathogenesis of BD is unclear, there has recently been growing evidence of oxidative stress in the pathogenesis of BD. Oxidants may have important roles in various biological reactions and may cause tissue damage. Iron is involved in the antioxidative system. It can catalyze the formation of potentially toxic free radicals. [1] Large amounts of iron are sequestered by ferritin in a non-toxic and readily available form in a cell. Ferritin expression is regulated by intracellular iron, inflammatory cytokines and oxidative stress. It has been reported that ferritin may have a new important regulator role of the immune system, playing a possible role in autoimmunity. Also, serum ferritin levels are elevated in some autoimmune disorders, particularly during disease activity. [3] There are a few reports investigating the levels of iron and/or ferritin in BD. [1],[2],[4] Odabas et al. found that patients with active BD had significantly higher ferritin levels and suggested that ferritin might be the activity criteria for BD. The other studies showed different outcomes about the levels of iron and/or ferritin in BD. [4] Ferritin levels in patients with BD and the control group and patients with active and inactive BD did not show significant differences. We assume that ferritin cannot be a diagnostic test and activity marker for BD . Decreased ferritin levels in females in the patient group may be related to the loss of iron via the menstrual cycle, abortus or delivery or nutritional status in females. We also found that patients with BD had significantly lower serum iron levels, although serum IBC and ferritin levels were not different in both the groups. Ferritin in inflammatory tissue contains more iron with increased inflammation. We assume that decreased serum iron levels in BD, as in chronic inflammation, may be due to defective iron release from the inflammatory tissue or reticuloendothelial cells to the erythroblast. [5] There are no studies investigating the relationship between iron and ferritin levels and clinical symptoms of BD in the literature. In our study, no relationship between iron levels and symptoms of BD was detected. However, serum ferritin levels were significantly higher in patients with PPL and thrombophelebitis. Consequently, the deficiency of iron may be seen in the patients with BD, as seen in chronic disease anemia. Even if ferritin is not a diagnostic and activity marker for BD, it may be contributory to some lesions of BD or those symptoms may cause an increased level of ferritin as an acute-phase reactant. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10029t1.jpg] [dv10029f1.jpg] [dv10029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}