 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
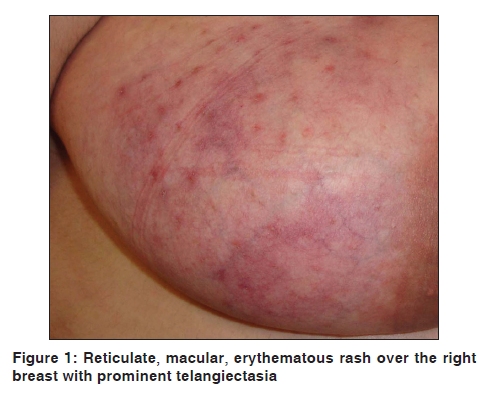
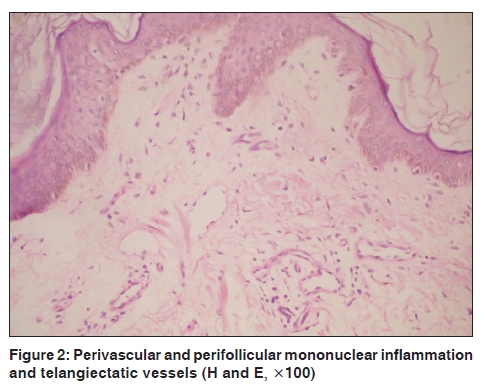
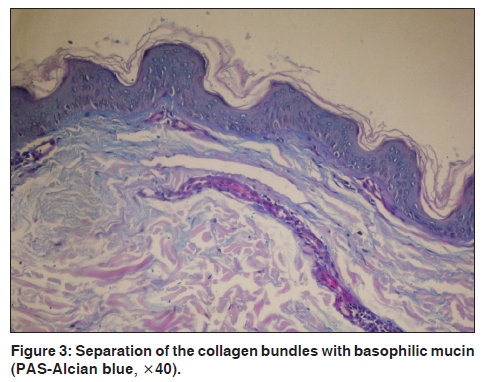
Indian Journal of Dermatology, Venereology and Leprology, Vol. 76, No. 1, January-February, 2010, pp. 86 Net letter Reticular erythematous mucinosis syndrome with telangiectasias Ayse Serap Karadag, Gulcin Guler Simsek1 Departments of Dermatology and 1Pathology, Ankara Kecioren Research and Training Hospital, Ankara Code Number: dv10030 PMID: 20061752 DOI: 10.4103/0378-6323.58697 Sir, Reticular erythematous mucinosis (REM) is a rare chronic dermatosis with a predilection for anterior and posterior trunk typically. It presents with reticular, macular lesions or erythematous papules and plaques. [1] Clinically, telangiectasia is not a characteristic of the REM. We report a case of REM with the presence of telangiectasias. A 38-year-old female was admitted to our unit for reticulate, macular, erythematous rash on bilateral breast skin for one year [Figure - 1]. Telangiectasias developed at the same time on these rashes. There was no history of sun-exposure and/or using medication. Her general physical examination was unremarkable. There was no lymphadenopathy or organomegaly appreciated on her examination. Laboratory investigations such as hemogram, liver and kidney function tests, thyroid hormone, antinuclear antibody, IgA, IgG, IgM, and serum complements levels were normal. Antibodies to native (single- and double-stranded) DNA were absent. Chest X-ray and abdominal ultrasonography were unremarkable. The microscopic examination of the skin biopsy revealed collagen fascicles with small amount of mucin and a few stellate fibroblasts, and perivascular and perifollicular mononuclear inflammation and telangiectatic vessels [Figure - 2]. The histochemical examination showed alcian blue staining positive mucin [Figure - 3]. Direct immunofluorescence test was negative for immunoglobulin and complement deposition. Based on physical examination and histopathological findings, REM was diagnosed. Topically, pimecrolimus twice a day was initiated. The skin lesions improved by the third month but they never completely resolved. There was no significant change in telangiectasia with treatment. REM is the primary and idiopathic form of cutaneous mucinosis. [1] There is predilection for young-aged females, but it may also occur in all ages and in both sexes. [2] Skin lesions usually occur in the central and upper chest, rarely arms; face and abdominal region can be involved. [1] In addition, clinically asymptomatic macular erythema, erythematous indurations, papule or plaques can be seen. [1] The etiology of the REM is still unclear. Some authors consider REM as a part of lupus erythematosus-like diseases spectrum due to its clinical findings, mucin deposition on histologic examination, progression after ultraviolet radiation exposure, and good responses to antimalarial drugs. [2] In 20% of the patients with REM, there is association with autoimmune diseases such as discoid lupus erythematosus, idiopathic thrombocytopenic purpura and diabetes mellitus. Associations with malignancies, thyroid diseases, monoclonal IgG kappa paraproteinemia, tumors, and myopathy have been reported as well. [1],[3] Antimalarial drugs, tacrolimus, pimecrolimus, pulsed dye laser, and UV-A1 radiation can be used in the treatment. [1],[3] Telangiectasias are small permanently dilated blood vessels. Photodamage, venous hypertension, trauma, radiodermatitis, and similar physical factors can cause telangiectasia. Corticosteroids, pregnancy, estrogen or progesterone, carcinoid syndrome, liver disease, and similar metabolic and hormonal factors, autoimmune connective tissue diseases, genodermatosis, vascular malformations and mycosis fungoides can result in telangiectasia as well. [4] Histologically superficial and mid-dermal vascular dilatation can be detected in the REM, but clinically it has been described only in two cases in the literature. [3],[5] Those cases were associated with essential thrombocytosis and lung carcinoma respectively. [3] Our case is due to telangiectasias in association with REM without any systemic diseases. References
Copyright 2010 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv10030f3.jpg] [dv10030f1.jpg] [dv10030f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}