 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 138-144 Original Article A retrospective study of intravenous sodium stibogluconate alone and in combinations with allopurinol, rifampicin, and an immunomodulator in the treatment of Indian post-kala-azar dermal leishmaniasis V. Ramesh, Joginder Kumar, Dhiraj Kumar, Poonam Salotra Department of Dermatology and Regional STD Center and Institute of Pathology (ICMR), Safdarjang Hospital and VM Medical College, New Delhi - 110 029, India Correspondence Address: Dr. V. Ramesh, D II/127 West Kidwai Nagar, New Delhi - 110 023, India, weramesh@hotmail.com Code Number: dv10038 PMID: 20228542 DOI: 10.4103/0378-6323.60553 Abstract Background and Aims: A retrospective analysis of treatment outcome
using recommended dose of sodium stibogluconate (SSG) alone and in combination
with other antileishmanial drugs in adults with post-kala-azar dermal
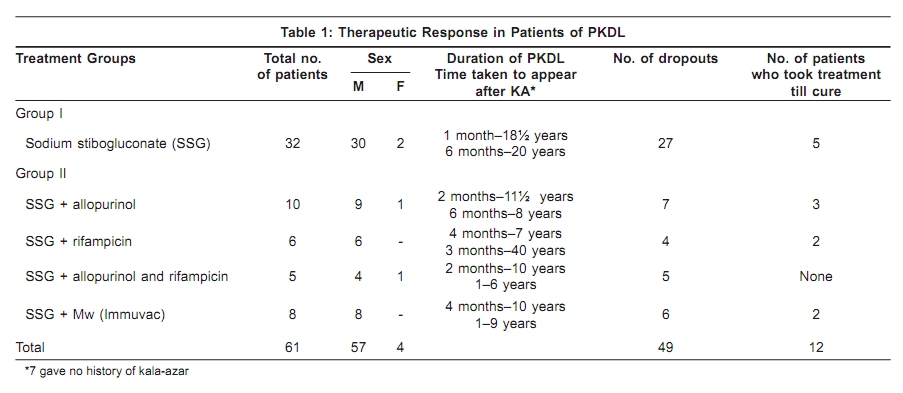
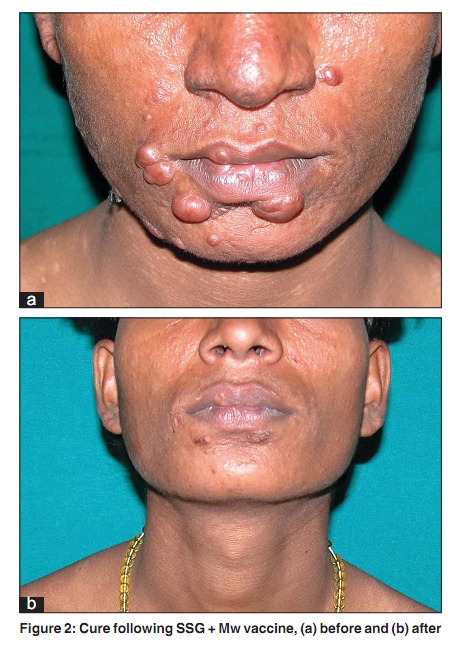
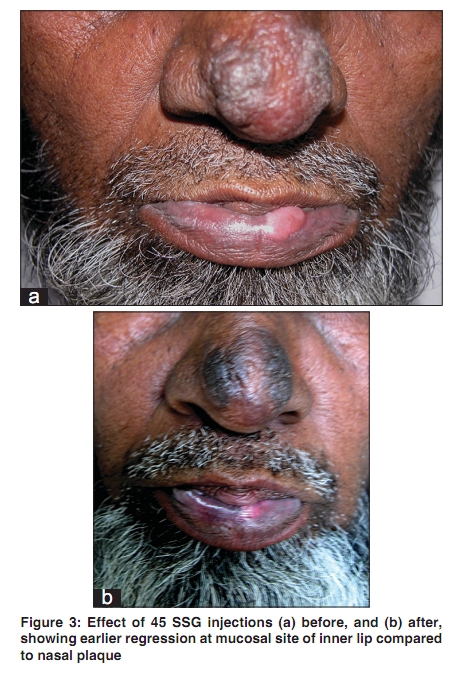
leishmaniasis (PKDL) attending as outpatients. Keywords: Allopurinol, kala-azar, Leishmania donovani, Mw vaccine, post-kala-azar dermal leishmaniasis, rifampicin, sodium stibogluconate, visceral leishmaniasis Introduction Post-kala-azar dermal leishmaniasis (PKDL) is an uncommon sequel seen after a variable period following treatment for kala-azar (KA) or visceral leishmaniasis caused by Leishmania donovani. Most of the patients have been from the Indian subcontinent comprising the eastern states of India and the neighboring countries of Nepal and Bangladesh, followed later by East Africa.[1],[2],[3],[4],[5] The transmission of infection in many of these areas being anthroponotic, PKDL is an important reservoir of the parasite in the spread of KA. In this report we have analysed the therapeutic response in PKDL seen over a period of 10 years in those who had been treated initially with only sodium stibogluconate (SSG) and later on patients in whom SSG was used in combination with either allopurinol or rifampicin, or both, and an immunomodulator. Methods Patients A total of 61 adults with PKDL, 57 men and 4 women between 18 to 65 years of age, from the year 1998 till 2007, were included in this retrospective study. All hailed from the state of Bihar endemic for KA in the eastern region of India and had left home to earn their livelihood. Pregnant or lactating women and patients with a predominantly macular presentation of PKDL have been excluded. History with reference to previous attack of KA, the treatment taken for KA, the time interval after which eruptions appeared and clinical examination were recorded. Routine blood and urinalysis, liver and renal function tests, serum amylase, x-ray chest, and electrocardiogram (ECG) were done prior to treatment. Slit-skin smears were performed in all patients and stained with Giemsa′s to note Leishman-Donovan bodies (LDB). Also, 4 mm punch biopsies were taken from the most infiltrated part of the face, usually the lower part of chin. Most of them declined admission and so all were treated as outpatients. Treatment groups To evaluate the therapeutic response the patients have been divided into two main groups. Group I (n = 32) were patients seen during first five years in whom SSG was given intravenously in the dose of 20 mg/kg/day not exceeding a total daily dose of 1 g (10 ml). The later patients comprising Group II (n = 29) were allocated in a phased manner during the next four years to any of the four combination regimens: SSG + allopurinol (n = 10) in the first year, SSG + rifampicin (n = 6) in the following year, SSG + allopurinol and rifampicin (n = 5) in the next year, and SSG + Mw vaccine (n = 8) in the fourth year. The dosage of orally administered drugs was allopurinol 800 mg/day in divided doses and rifampicin 15 mg/kg varied from 750 mg to 900 mg/day. Mw vaccine (Immuvac, Cadila Pharmaceuticals, Ahmedabad, India), an immunomodulator containing heat-killed Mycobacterium w 0.5 x 109 cells in each dose of 0.1 ml, was given intradermally over both deltoid regions, 0.1 ml at each site on first visit, and subsequently one dose of 0.1 ml was repeated over either deltoid area every fortnight to a total of five doses. The patients in both groups were seen every fortnight for the first month and later monthly, except those on vaccine therapy who attended fortnightly till completion of five doses. Liver and renal function tests, serum amylase, and ECG were done monthly and at the end of therapy. Criteria of cure Punch biopsy from face was repeated when all clinical evidence of disease activity seen as induration and erythema had subsided leaving normal appearing skin. After completion of therapy the patients reported for follow-up every 6 months till the end of three years. Results Clinical and Histopathologic Details All the patients had mixed or polymorphic PKDL characterized by indurated lesions seen as erythematous to dull red papules, plaques and papulonodules, and hypochromic macules. The face was often involved followed by the trunk, extremities, and the genital skin. Mucosal lesions were seen in 20 patients. Fifty-four patients gave a past history of having KA, out of which 53 had been treated with SSG, and one had been given amphotericin B. Seven gave no history of KA, five in Group I and two in Group II. In five of these the face was mainly affected with occasional papules on upper back. As seen in [Table - 1], the duration of PKDL ranged from one month to 18½ years in Group I; and two months to 11½ years in Group II. On the whole, skin lesions appeared three months to as long as 40 years after treatment for KA. Histopathology was similar to that described earlier.?[2],[3] It showed a homogeneous infiltrate composed of lymphocytes, plasma cells, and macrophages. Lymphocytes and plasma cells were the predominant cells amidst which the macrophages were scattered. The infiltrate was dense in the upper and mid dermis in biopsies from indurated sites and occupied the entire dermis in papulonodular lesions. Fite-Faraco stain for acid-fast bacilli was negative in all patients. Giemsa′s stain revealed LDB in slit-skin smears from 28 patients. In the 12 biopsies taken from patients who had taken therapy till cure, histopathology revealed a thin to normal epidermis and little or no signs of inflammation in the dermis. Effect of therapy In Group I, only five of 32 patients were able to complete the recommended 120 injections intravenously within 150– 170 days. In Group II, three out of ten in the SSG + allopurinol category were considered cured after 95 injections within 110 days; two of six achieved cure in the SSG + rifampicin category after 110 injections of SSG in 135 days [Figure - 1]a and b; but none of five in the SSG + rifampicin and allopurinol category could continue injections beyond 1½ months; an 18-year-old adolescent male who stopped SSG after a month continued rifampicin and allopurinol with subsidence of disease after 16 months. In the last group where SSG was combined with Mw vaccine, two attained cure, one with 95 injections over 115 days. [Figure - 2]a and b The other was a drop-out from Group I who relapsed four years after taking 55 injections of SSG and had attained cure after 135 injections of SSG spread over 168 days along with Mw. As described before,[4] the lesions had started showing signs of subsidence in both groups by three to four weeks. The mucosal lesions were the first to show signs of regression followed by those over the skin [Figure - 3]a and b. In 10 cases, 4 from Group I and 6 from Group II, evidence of regression could be seen at the end of a fortnight and seven of them were patients without a previous history of KA. The patients were reassured that the hypochromic macules would take time to repigment after completion of therapy. None of the patients showed ECG abnormalities during therapy. Renal function tests and serum amylase remained within normal limits. Two of four in Group I, who attained cure, showed mildly elevated liver enzymes at the end of treatment. Among the patients who were dropouts and did not complete therapy till cure, 12 out of 27 in Group I and 10 out of 22 in Group II experienced subsidence of papulonodules and plaques after 60 injections [Figure - 4]a and b. Side-effects of Treatment In both Groups I and II, the interruptions in SSG therapy had resulted from bodyaches, giddiness, metallic taste, loss of appetite, and severe joint pains. Frequent injections left cord-like structures replacing patent veins due to thrombophlebitis. Few experienced vomiting and febrile episodes, and one in the SSG + allopurinol category had postural hypotension. Practical difficulties also arose due to poor availability of SSG, accessing new veins, and seeking a cooperative medical person to administer them. At times, SSG had to be taken intramuscularly. Group II patients continued oral medication during the injection-free rest periods. Follow-up Following cure, four of five patients in Group I completed two years of follow-up and one did not show up after a year. None of them showed signs of relapse. Four out of seven in Group II remained normal after two years of follow-up. One in the SSG + allopurinol did not return after six months of follow-up and both patients in the SSG + Mw vaccine category have completed one year of follow-up with no signs of renewed activity of PKDL. Discussion The recommended dose of SSG in Indian PKDL is 20 mg/kg/day to a maximum of 850 mg (8.5 or 10 ml depending on whether antimony concentration in preparation is 100 or 85 mg/ml) for 120 days;[1] a subsequent study showing that 20 mg/kg/day could be given without an upper limit.[5] Studies in Indian PKDL are few and large series[6],[7] in which SSG was administered intramuscularly daily described no serious changes in ECG and the patients were able to complete therapy even when the duration was extended to 200 days to combat refractoriness and prevent relapse. Arthralgia, pain and swelling at the site of injection had to be managed with analgesics, hospitalization, and brief discontinuations in the therapy. Our first experience with intramuscular SSG up to a maximum of 1 g/day in 18 patients had been similar.[4] To improve compliance, orally administered drugs, ketoconazole[8] and allopurinol,[9] have been tried independently and were found effective in PKDL, but the response was slow, showing that their antileishmanial effect was weak. Allopurinol has shown synergism when given along with SSG and the combination has been used in relapse of PKDL following the SSG therapy.[10] Experience with African PKDL seen in Ethiopia, Kenya, and Sudan[11] has been different from that in Indian PKDL. A highly variable course extending from spontaneous regression to those requiring treatment with SSG has been observed. They have been cured with a month′s course of SSG which has been the duration employed in some studies.[12] but few behave akin to Indian PKDL requiring two to four months of treatment or repeated courses of SSG, necessitating shorter regimens with liposomal amphotericin B 2.5 mg/kg/day as intravenous infusion for 20 days.[13] Arthralgias have also been noted in patients cured after a 30-day course of SSG[14] and in a poor responder to SSG ketoconazole was given without success, the lesions clearing after a month only when SSG dose was raised to 30 mg/kg/day. These observations indicate that SSG is the chief component in both Indian and African PKDL. In a recent study,[15] over half the number of patients were cured with a 40-day course of parenteral SSG not exceeding 850 mg/day, almost never seen in Indian PKDL. Data on the experience and difficulties of prolonged administration of SSG in African PKDL have yet to be published. In this retrospective study, all patients had polymorphic lesions and hailed from Bihar. Most were young adults engaged in physical work for livelihood and desired to take treatment as outpatients. Since LDB are not visualized in a significant number patients, the diagnosis of PKDL as outlined before[2],[3] was based on clinical picture, history of having suffered from KA in the past or coming from a KA-endemic area, exclusion of other dermatoses, histopathology, and response to therapy. Predominantly macular presentations, though uncommon, were excluded from the study as macules usually show minimal abnormalities on histopathology and persist for long after completion of therapy, rendering assessment difficult. The intravenous route was preferred, which was comparatively less painful than the intramuscular one, and had not been tried routinely in PKDL. They managed to take the injections regularly without break for a month or with occasional breaks for two months, but few managed to take till cure. In order to reduce the number of injections, it was combined in Group II with other drugs namely allopurinol, rifampicin, both allopurinol and rifampicin, and Mw vaccine. Mw vaccine is derived from a nonpathogenic, saprophytic, rapidly growing Mycobacterium,[16] and a chance observation[17] of its efficacy in PKDL in the mid-nineties, led us to try it along with SSG. It is currently marketed as an immunomodulator for augmenting Th1 response of the host in many conditions. Only seven out of 29 patients managed to take therapy till cure in Group II, none of them being from the category in which SSG was used along with rifampicin and allopurinol. These figures are almost similar to Group I, where five out of 32 had taken therapy till declared cured. Those who had completed 60 injections showed similar pattern of regression of lesions as observed in a previous study,[18] and this applied to both groups, the mucosal ones responding earlier than skin lesions. Patients without a previous history of KA had relatively localized disease at presentation and showed an earlier therapeutic response after two weeks of treatment. However, during the latter part of therapy, erythema and induration as compared to Group I, had subsided in a shorter time in the three categories in Group II, where patients had attained cure. It was earlier in those where SSG was given along with allopurinol and Mw vaccine respectively, followed by SSG plus rifampicin. The reduction in the number of injections varied from 10 to 25 compared to the standard regimen. This would at best shorten therapy by a month and since most patients could not endure injections beyond two months, no significant benefit was foreseen. The patients in both groups could not take SSG injections without interruptions; while those in Group II continued the oral drugs. One patient in the SSG plus Mw category required 135 injections to achieve cure, the highest in this study. He was also one of seven patients reported elsewhere in a study on in vitro susceptibility of L. donovani to SSG, found to harbor parasites susceptible to antimony at high concentrations.[19],[20],[21] Eleven out of 12 patients completed between 1– 2 years of follow-up with no signs of relapse. The PKDL patients in the current report were otherwise healthy, refused hospitalization, and found treatment worse than disease owing to recurring physical and practical problems which accounted for a large number of dropouts. The side-effects were due to SSG administration. Arthralgias and bodyaches proved to be the worst, affecting daily work. Inflamed and sclerosed veins forced some to choose the intramuscular route. In previous studies, brief injection-free rest periods[4],[7] and longer interruptions with cyclical regimens[20] have been allowed to facilitate the therapy. Attempt to reduce duration of therapy using ketoconazole along with SSG has been unrewarding.[18] The recently recommended treatment of KA with SSG for a month is cost-effective,[21] but if extended as in PKDL rheumatic side-effects would seriously hinder compliance.[22] In a report of 22 PKDL patients from Nepal, these side-effects had commenced in 50% of patients within 1– 2 weeks of the start of SSG therapy.[23] Neuritic symptoms have also been reported.[8] None of our patients had ECG abnormalities or evidence of liver, renal, and pancreatic dysfunction. Pancreatitis, mainly subclinical and unusually rare in PKDL, has occurred during SSG therapy for cutaneous leishmaniasis as evidenced by increased serum amylase or lipase levels associated with signs or symptoms of abdominal discomfort, but patients could complete treatment.[24] A recent study inferred that both hyperamylasemia and raised liver transaminases are clinically insignificant and not deterrents to treatment.[25] Fatalities due to pancreatitis have occurred in those coinfected with HIV.[26] Other ways of reducing the volume of SSG injected by increasing concentration of antimony may minimize local side-effects. Unfortunately at levels above 100 mg/ml SSG tends to supersaturate forming crystals and precipitates. As inpatients, intravenous SSG 10 mg/kg/day (5 ml) for 120 days along with rifampicin 900 mg/day, has yielded satisfactory results.[27] Alternatively, duration of therapy could be shortened by immunotherapy in addition to the recommended dose of SSG. However, our results with Mw vaccine were less impressive. Using an L. major-derived vaccine with SSG injections given for 40 days, 87% of PKDL patients in Sudan attained cure after with no relapses as opposed to 53% in the group where only SSG was given in which two relapsed.[15] Liposome entrapped SSG (Pentostam) achieved better results with low doses in L. donovani-infected mice[28] indicating enhanced drug delivery, but this was not popularized for wider application. Conclusion Irregular and intermittent therapy with SSG has been said to promote emergence of drug resistance[29] and is a potential possibility in PKDL[19] since the majority of patients are unable to complete therapy, or do so with intervening periods of rest. A little over a decade ago we had also documented that PKDL may be partly responsible for the spread of KA refractory to antimony reported during the eighties.[30] Till date there is no acceptable multi-drug formulation recommended for PKDL. Though the number of patients recruited in each group is small, it is evident that the combinations tried by us along with SSG are not robust enough in terms of compliance and efficacy compared to SSG alone. As the duration of treatment in PKDL is likely to be longer, oral administration is preferable. Currently miltefosine, the only drug to fulfill this requirement, is beset with high cost of therapy and is not freely available. The results of drug trials in PKDL are awaited to determine the optimum dose and duration for miltefosine. Poverty and leishmaniases have been said to constitute a mutually reinforcing cycle[31] and any acceptable form of treatment must not overlook this aspect. Till then antimonials appear to be the Hobson′s choice in the treatment of PKDL with amphotericin B in reserve for refractory or antimony-resistant patients. Acknowledgments We are grateful to Dr. Subhasri Bandyopadhyay, Medical Advisor, Albert David Limited, Kolkata (Calcutta). Research fellowship to Dhiraj Kumar by the Council of Scientific and Industrial Research, Government of India is acknowledged. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10038f2.jpg] [dv10038f4.jpg] [dv10038f3.jpg] [dv10038t1.jpg] [dv10038f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}