 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
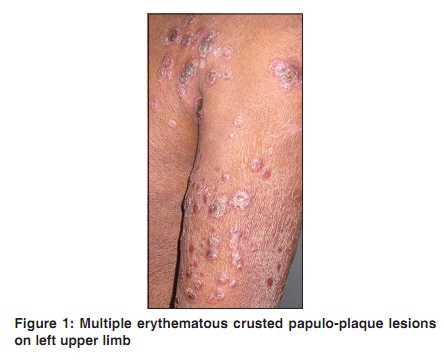
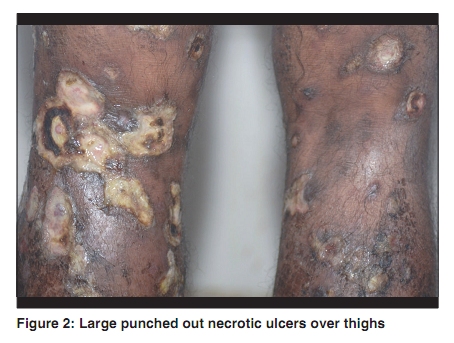
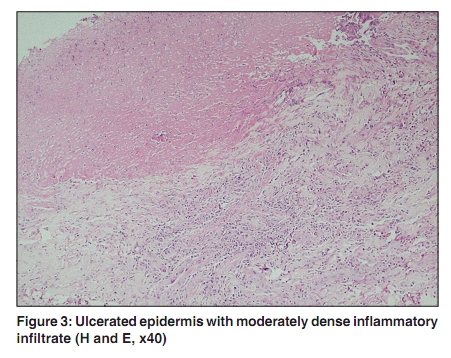
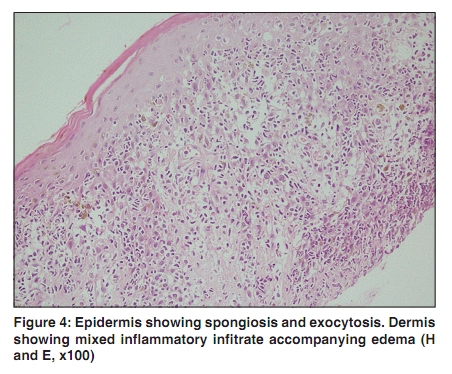
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 172-175 Case Report Pityriasis lichenoides with ulceronecrosis and hyperthermia: A rare variant of pityriasis lichenoides et varioliformis acuta Sarvjit Kaur Virdi, Amrinder Jit Kanwar, Uma Nahar Saikia Departments of Dermatology, 1Pathology, PGIMER, Sector 12, Chandigarh - 160 012, India Correspondence Address: Dr. Sarvjit Kaur Virdi, #1090 Phase 3B2, Mohali, Sector 60, Punjab - 160 059, India, ijssohal@yahoo.com Code Number: dv10044 PMID: 20228548 DOI: 10.4103/0378-6323.60572 Abstract Pityriasis lichenoides with ulceronecrosis and hyperthermia (PLUH) is a severe variant of pityriasis lichenoides et varioliformis acuta that is characterized by high fever and papulo-necrotic skin lesions. We report the case of a 49-year-old male with typical features of PLUH along with an unusual manifestation of extensive skin necrosis including involvement of the intertriginous regions. Systemic administration of corticosteroids and antibiotics did not help to control the disease and the patient succumbed to death due to its fulminant nature.Keywords: Pityriasis lichenoides, ulceronecrosis, hyperthermia Introduction Pityriasis lichenoides (PL) is an uncommon, acquired spectrum of skin conditions that poses various challenges to patients as well as clinicians. It is a difficult and debatable disorder to diagnose, categorize and treat. Besides these inherent obstacles, PL merits awareness because of its potential to progress to cutaneous lymphoma[1] or an ulceronecrotic presentation, both of which carry a significant risk of mortality. The scope of PL presentations is delineated along a continuum of multiple variants including pityriasis lichenoides et varioliformis acuta (PLEVA), pityriasis lichenoides chronica (PLC), and febrile ulceronecrotic Mucha-Habermann disease (FUMHD), also known as pityriasis lichenoides with ulceronecrosis and hyperthermia (PLUH). We report a 49-year-old male patient with fulminant course of pityriasis lichenoides with ulceronecrosis and hyperthermia with ultimately fatal outcome in a short course of time. Case Report A 49-year-old male, milk vendor by occupation, presented with erythematous papules and crusted plaques all over the body and ulcerations in the oro-genital tract of 15 days duration. The lesions started as multiple, erythematous, papulo-plaques on the upper limbs (involving axillae, palms and soles), trunk, lower limbs and face including nasal cavity and upper eyelids. They progressed in number and size to form large ulcerated plaques with thick crusting. Simultaneously, ulcerations appeared in the oral cavity and on the genitalia. The disease severity incapacitated him from his routine activities. The illness was associated with high grade fever. There was no history of drug intake or sore throat prior to the onset of illness. There were no associated complaints of any joint pains, dysuria, respiratory or abdominal problem. There was no history of any extramarital contact. There was no similar illness in the family. He was not a known diabetic or hypertensive. On general physical examination, he was average built, nourished and febrile (1010 F) with tachycardia at the time of examination. There were two to three non-tender, discrete, mobile superficial inguinal lymph nodes on right side. Systemic examination did not reveal any finding. On detailed cutaneous examination, around 25-30% of body surface area was involved with bilateral and symmetrical distribution of the lesions on upper limbs, trunk and lower limbs [Figure - 1]. The lesions were seen as discrete and coalescent erythematous and edematous papules. Most of the lesions showed pustulation and hemorrhagic crusting. These lesions enlarged to form punched-out ulcers with well-defined margins varying in size from 1-10 cms with necrotic tissue on the base [Figure - 2]. Ulcerations with hemorrhagic crusting were present at the margins of the nose as well as on the upper and lower lids. Oral mucosa showed multiple superficial and deep ulcers at angles of the lips, tongue and buccal mucosa. Genital mucosa showed multiple ulcers around 1 cm in size, well-defined, non-tender and non-indurated on the prepuce and glans penis with associated phimosis. Palms and soles showed multiple well-defined erythematous maculopapular and pustular lesions. Nails were discolored with longitudinal ridging. Hair was normal. There was no enlargement of the peripheral nerves. Based on the clinical presentation, the differential diagnosis of erythema nodosum leprosum (ENL) necroticans, malignant syphilis, ecthyma gangrenosum, Wegeners granulomatosis and ulceronecrotic variety of PLEVA were kept. On laboratory investigation, the haemogram showed leucocytosis (total leucocyte count of 14.3X109/L) with normal differential count and peripheral blood film picture. Other parameters such as erythrocyte sedimentation rate, C-reactive protein, random blood sugar, routine urine examination, renal function tests were found to be normal. Liver function tests showed raised enzyme levels (ALT 109 IU, AST 81.23 IU, alkaline phosphatase 347 U/L). VDRL, TPHA, viral markers (hepatitis B and C) and HIV were non-reactive/ negative. There were no giant or acantholytic cells from oral cavity. Gram stain from the lesions on the body showed pus cells and no microorganisms. Slit-smear examination did not show any AFB. Blood, urine and throat cultures were negative. Both ANA and ANCA (against both proteinase 3 and myeloperoxidase) were negative. Chest X-ray, ECG and ultrasound abdomen were normal. Skin biopsy from the ulcer [Figure - 3] showed necrotic epidermis with moderately dense inflammatory infiltrate in the dermis. Skin biopsy from the raised erythematous and oedematous papules [Figure - 4] showed moderate exocytosis and spongiosis in the epidermis. Dermis showed dense inflammatory infiltrate composed mainly of lymphocytes around the blood vessels accompanying edema and infiltration of the vessels with inflammatory infiltrate at many sites indicating small vessel vasculitis suggestive of PLEVA. Direct imunofluorescence study demonstrated deposition of fibrinogen on deep dermal vessel wall. On the basis of the clinico-pathological correlation, the final diagnosis of ulceronerotic variant of Pityriasis lichenoides et varioliformis acuta was made. The patient was treated with antibiotics and high dose of oral corticosteroids as well as symptomatic treatment. This was followed by only mild to moderate improvement. The patient reported in follow-up with exacerbation of the disease. On re-admission, approximately six weeks later, new lesions continued to develop, intravenous antibiotics and pulse therapy was instituted and nursing care augmented. But the patient succumbed to death secondary to acute respiratory distress syndrome and multisystem failure. Discussion Pityriasis lichenoides with ulceronecrosis and hyperthermia (PLUH) represents a fulminant and potentially lethal variant of pityriasis lichenoides et varioliformis acuta (PLEVA). In 1916 Mucha and in 1925 Habermann reported an acute form of pityriasis lichenoides characterized by the abrupt onset of papulovesicular eruptions and described it as pityriasis lichenoides et varioliformis acuta (PLEVA) or Mucha-Habermann disease. Later, in 1966, Degos reported a rare febrile ulceronecrotic variant of PLEVA. PLEVA and PLUH occur most commonly in children, adolescents and young adults. The cutaneous lesions in PLEVA are usually asymptomatic, but may be pruritic and may heal with scarring. These patients rarely have systemic signs. PLUH on the other hand, often starts out as classic PLEVA but goes on to develop widespread ulceronecrotic lesions and is associated with a high mortality rate particularly in adults and immunocompromised patients. Till date only 31 cases of PLUH have been reported in English literature.[2] Although the exact etiology for PLUH is unknown, several reports have suggested the possibility of hypersensitivity to an infectious agent. The elevation of microbe-specific antibody titers, deposition of immune complexes in dermal vessels, familial outbreaks and associated constitutional symptoms have been offered as potential evidence for infectious causality. Auster et al. reported adenovirus isolated from urine to be the possible etiologic agent in PLUH and interstitial pneumonitis in their patient.[3] A patient described by Hoghton et al.[4] had lymphocytic myocarditis consistent with viral causation; De Cuyper et al.[5] have described a patient who had respiratory infection before the abrupt onset of disease. Puddu et al.[6] had positive blood cultures for Staphylococcus aureus and Pseudomonas aeruginosa. They also detected circulating IgM immune complex and deposition of C3 in dermal vessels. Many different infectious agents have been implicated in pathogenesis, but there has been no consistent finding so far.[7] The reported etiologic pathogens include EBV, HIV, parvovirus B19, adenovirus, Staphylococcus aureus and group A Streptococcus on throat cultures, Mycoplasma pneumoniae and Toxoplasma gondii.[8] Transition of PLEVA to PLUH has been associated with increase levels of TNF-alpha in one patient.[9] Another postulated mechanism for PLEVA′s pathogenesis is lymphocytic proliferation. Lopez-Estebaranz et al, however, implied that PLUH represents an inflammatory disorder rather than a T-cell lymphoproliferative process as they did not detect abnormalities in T-cell receptor gene analysis of DNA from skin lesion and peripheral blood.[10] Our patient had extensive skin and mucosal involvement characterized by great number of large, coalescent ulcerations. However, no infective agent was found from the skin, throat, blood or urine samples. In the biopsy specimen, lymphocytic infiltrate within and around the vessel wall was seen. Direct immunofluorescence study demonstrated deposition of fibrinogen on deep dermal vessel wall. Results of slit smear examination, serologic tests for syphilis, antinuclear and anti-DNA antibodies and antineutrophil cytoplasmic antibodies against both proteinase 3 and myeloperoxidase were negative. Immunohistochemical studies and TNF-alpha levels could not be performed due to lack of facilities. Management of PLUH is controversial and a considerable number of therapies have been tried. These include systemic corticosteroids, antibiotics, acyclovir, dapsone, methotrexate, psoralen plus ultraviolet A, TNF-alpha inhibitors (such as infliximab and etanercept). A combination of these agents has been tried in some patients. In our patient, systemic coticosteroids in dosages greater than 1 g/kg per day, along with oral and intravenous antibiotics, were used. However, despite the best efforts, no improvement was seen. The patient was then administered dexamethasone pulse therapy due to rapid flare up of the lesions. Despite corticosteroid therapy and supportive therapy, the fulminating course of the disease with multisystem failure led to death of the patient. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10044f3.jpg] [dv10044f1.jpg] [dv10044f4.jpg] [dv10044f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}