 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
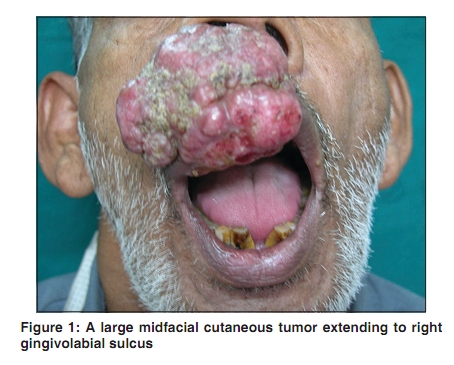
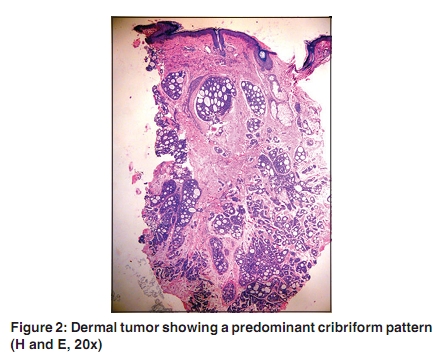
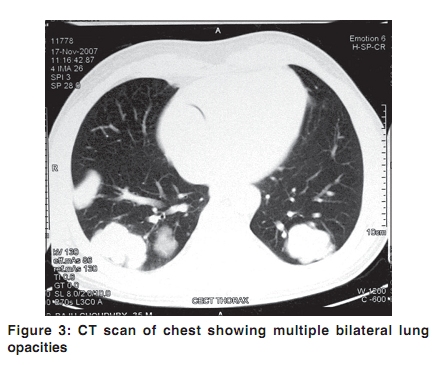
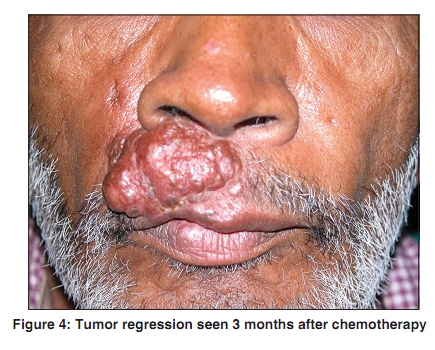
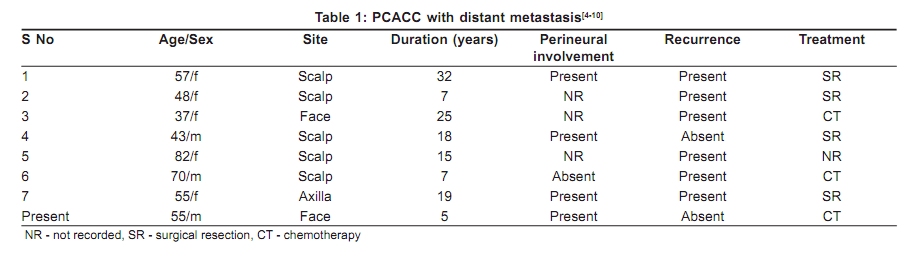
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 176-179 Case Report Primary cutaneous adenoid cystic carcinoma with distant metastasis: A case report and brief literature review Avninder Singh, V. Ramesh1 Institute of Pathology-ICMR, 1Department of Dermatology, Safdarjung Hospital, New Delhi, India Correspondence Address: Dr. Avninder Singh, Institute of Pathology, ICMR Safdarjung Hospital Campus, New Delhi - 110 029, India, dravninder@yahoo.co.in Code Number: dv10045 PMID: 20228549 DOI: 10.4103/0378-6323.60573 Abstract Primary adenoid cystic carcinoma (PCACC) of skin is a rare tumor, and those who show distant metastasis are even rarer. We report a case of PCACC on the face of a 55-year-old man who showed bilateral lung metastasis and on palliative chemotherapy showed significant regression of the primary tumor. The patient was alive at a 15-month follow-up. A brief literature review of the eight cases including ours is described.Keywords: Adenoid cystic carcinoma, metastasis, skin Introduction Primary cutaneous adenoid cystic carcinoma (PCACC) is a rare but well-documented entity with 62 cases reported in the literature. [1] We report a case of PCACC with pulmonary metastasis in a 55-year-old male and review the literature for reported cases of PCACC with distant metastasis. To the best of our knowledge, this is the eighth case of PCACC with distant metastasis. Case Report A man aged 55 years presented with a growth arising from the skin on infranasal area above the lip of 5-years duration and generalized scaly lesions for 10-year duration that were exacerbated during winters. On general examination, he was found to be moderately built, not anemic or jaundiced. A firm to hard 5 cm × 5 cm midfacial mass with irregular margins was arising from below the right nasal vestibule with firm consistency, non-tender, and extending to right upper gingivolabial sulcus and had no connection with the inner lip mucosa [Figure - 1]. The regional lymph nodes were not enlarged, nor were any other swelling felt elsewhere. CT scan of head and neck did not show any other mass lesion. Systemic examination was normal except for basal crepitations of chest. Blood, urinalysis, and abdominal ultrasound revealed no abnormality. A punch biopsy of the tumor showed a dermal tumor arranged predominantly in a sieve-like pattern, composed of cords and strands of basaloid cells with a cribriform, glandular, and cystic arrangement [Figure - 2]. The tumor showed an area of perineural involvement. The tumor nests were surrounded by a eosinophilic hyaline basement membrane-like material that was periodic acid-Schiff (PAS) positive and diastase resistant. The cystic pseudoglandular spaces were filled with secretions that were PAS negative and Alcian blue positive. The tumor cells showed mild pleomorphism and occasional mitosis. Immunohistochemistry showed positive reaction with a epithelial membrane antigen (EMA), pan-cytokeratin, and focal positivity for S-100. Immunohistochemical expression for the carcinoembryonic antigen (CEA) was demonstrated in the ductal lumina and also strong immunopositivity for c-kit was seen. The history, otorhinolaryngology examination, and imaging of head and neck excluded the possibility of salivary gland origin. A diagnosis of PCACC was entertained. Wide surgical excision was planned, but the patient refused surgical intervention. The initial work up had shown bilateral multifocal opacities on chest X-ray. Contrast enhanced CT chest revealed multiple lobulated mass lesions in both lungs showing contrast enhancement. The largest lesion measured 4.3 × 3.5 cm in size with no evidence of necrosis or calcification [Figure - 3]. The findings were suggestive of metastasis. Simultaneous CT-guided fine needle aspiration done from one of the peripheral lung deposits showed a cellular smear with plenty of spherical globules, adherent round to oval clusters of tumor cells, and finger-like stromal hyaline fragments suggestive of adenoid cystic carcinoma. The diagnosis of PCACC with pulmonary metastasis was entertained. He was given 2 cycles of palliative chemotherapy consisting of cisplatin 100 mg on day 1 in combination with 5-fluorouracil from days 1-3. The tumor remarkably regressed to its initial site of origin over the skin within 10 weeks [Figure - 4]. At a 15-month follow-up there was no recurrence, but he had cachexia. Discussion PCACC is a rare but distinctive tumor of skin first described in 1975 by Boggio. [2] Although its histogenesis is still not clear and no universally agreed predisposing factor is known, it is characterized by a cribriform pattern and perineural involvement. The tumor is commonly seen in organs like salivary gland, lungs, breast, esophagus, cervix and ceruminous, and lacrimal glands. When metastasis from ACC of other organs is excluded, PCACC is the most probable diagnosis. PCACC affects middle aged and elderly with a mean age of 58.1 years and has a predilection for women with male: female ratio of 4:1.Scalp is the favored location. The average duration of the tumor prior to diagnosis is 9.8 years with a tumor size ranging from 0.5 to 8.0 cm. [3] The patients usually present with a slowly expanding firm skin-colored nodule that typically shows an indolent and progressive clinical course. Microscopically PCACC is composed of islands and cords of basaloid cells arranged in solid, cribriform, or tubular patterns embedded in a loose fibromucinous stroma. Tumor is situated in the mid and deep dermis and shows no connection with the epidermis. Tumor shows infiltrating margins and perineural involvement in one half. The tumor cells produce basal lamina that eventually becomes hyalinized and is PAS positive, diastase resistant. The adenoid spaces or pseudolumina accumulate hyaluronic acid and sulfated mucins. Immunohistochemical reactivity for EMA, cytokeratin, S-100, and actin is usually seen. The important histopathological differential diagnoses includes adenoid basal cell carcinoma which should be differentiated by the presence of peripheral nuclear palisading, stromal retraction clefts epidermal connection, and by the absence of perineural spread. These are usually CEA and S100 negative. Mucinous carcinoma of skin may show cribriform areas and mimic PCACC and is excluded by the presence of pools of mucin that stain strongly for sialomucins. Another recently described distinct cutaneous neoplasm with the variegated histological appearance that too may show the cribriform areas is the polymorphous sweat gland carcinoma and needs to be excluded. Rarely, metastatic carcinomas from sites such as breast, pancreas, and lungs may display a cribriform pattern and have to be excluded by clinical examination and demonstrate the presence of PAS-positive epithelial mucins and specific immunohistochemical markers. An indolent but progressive course is characteristic of this tumor, and local recurrence is seen in more than 50%. [3] Lymph node and distant metastasis are rarely seen. The literature review shows only seven cases of distant metastasis all of which occurred in lungs [4],[5],[6],[7],[8],[9],[10] [Table - 1]. Though PCACC is histologically indistinguishable from other ACC, and its clinical behavior is similar, but the rate of pulmonary metastases of PCACC is lower than extracutaneous ACC. [11] Pappo et al [7] studied the growth rate of lung metastasis by serial chest X-rays and demonstrated that the doubling time of lung metastasis in PCACC is longer than any other doubling time of lung metastasis previously reported, thereby suggesting that they are extremely slow growing tumors and a longer survival can be expected. Surgical excision of the primary lesion with wide tumor-free margin is the treatment of choice. Due to few reports on lymph node metastasis, some authors have suggested regional lymph node dissection along with surgical excision as a reasonable treatment option for large lesions. Irradiation should be an adjunct to surgery especially when there is doubt about complete excision. Complete tumor regression by chemotherapy, as in our case, has been previously documented. [6] To conclude, PCACC are rare skin tumors in adults with predilection for scalp and face. Chest examination should invariably be done, as these tumors may have propensity for pulmonary metastasis. However, the number of these is very few and follow-up details are too short to derive any definite conclusions about their clinical behavior. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10045f4.jpg] [dv10045f3.jpg] [dv10045t1.jpg] [dv10045f1.jpg] [dv10045f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}