 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
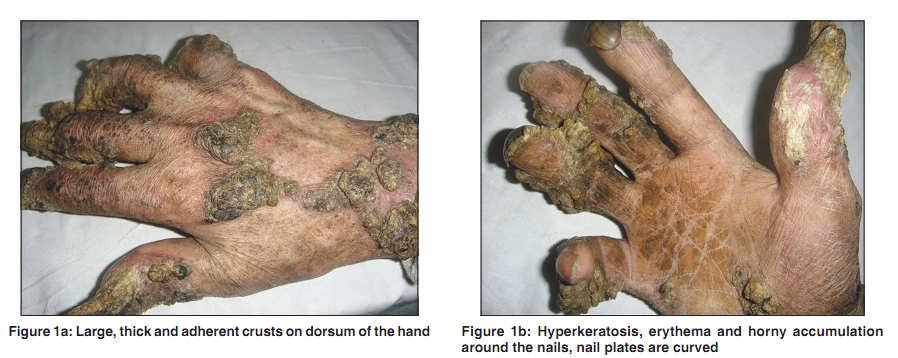
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 180-181 Images in Clinical Practice Lupus vulgaris: An atypical presentation Iffat Hassan, Mashkoor Ahmad, Qazi Masood Department of Dermatology, STD & Leprosy, Govt. Medical College and Associated SMHS Hospital, Srinagar-Kashmir (J&K), India Correspondence Address: Dr. Iffat Hassan, Department of Dermatology, STD & Leprosy, Govt. Medical College and Associated SMHS Hospital, Srinagar-Kashmir (J&K), India, hassaniffat@gmail.com Code Number: dv10046 PMID: 20228550 DOI: 10.4103/0378-6323.60571 A 60 year old male, farmer by occupation, presented with one year history of an asymptomatic lesion on his right hand. The lesion started as a red nodule on the tip of the thumb one year back and gradually involved both sides of his hand. Cutaneous examination revealed an area of hyperkeratosis on the right palm and large thick adherent crusts on an erythematous base on the dorsal aspect [Figure - 1]a. The nail plates were curved and the keratinized material around the nails was shaped like cutaneous horns [Figure - 1]b. There was erythema, scarring and atrophy in between the areas of hyperkeratosis. A well defined plaque with similar crusting and erythema was present on the right upper arm. There was no regional or generalized lymphadenopathy. There was no systemic complaint. The general physical and systemic examinations were within normal limits. Histopathology of lesional skin from hand revealed mild hyperplasia of epidermis with multiple caseating granulomas containing Langhans giant cells and epitheloid cells in the dermis. A tissue smear for LD bodies was done to rule out cutaneous leishmaniasis and it was negative. PCR from the lesional skin specimen from hand was positive for mycobacterium tuberculosis. Chest x-ray revealed bilateral apical cavities in lungs and sputum was positive for acid fast bacilli. Mantoux test was strongly positive. There was no past history of anti-tubercular treatment. The patient was diagnosed as a case of lupus vulgaris with underlying pulmonary tuberculosis and was put on category I, DOTS regimen for six months. There was dramatic improvement in the skin lesions after six weeks of treatment [Figure - 2]. There was marked reduction in erythema, crusts and keratinization around the nails. Lupus vulgaris is a progressive form of cutaneous tuberculosis occurring in a person with moderate to high degree of immunity. It develops as a result of direct inoculation, direct extension from an underlying organ or by lymphatic spread. Rarely, it can occur as a result of haematogenous spread from an infective focus. The common sites of involvement are head and neck followed by arms and legs. The lesion is usually single and starts as a tiny reddish-brown nodule, which later becomes raised and infiltrated. Clinically lupus vulgaris presents in five general patterns: plaque form, ulcerative and mutilating form, vegetating form, tumor like form and papular and nodular form. In plaque form, there is well defined border with little infiltration and scaling and minimal scarring in the centre. In ulcerating form, crusts form over the areas of necrosis and scarring and ulceration predominates. Vegetating form is characterized by marked ulceration and extensive infiltration. The tumor-like form presents as a deep infiltration in the form of soft and smooth grouped nodules or a reddish-yellow plaque. In papular and nodular type, multiple lesions occur in disseminated pattern. Besides these clinical types of lupus vulgaris, atypical forms are becoming more common. In our case, large thick adherent crusts on the dorsum of hand with minimal ulceration were present. There was no destruction of the underlying tissue. The areas of hyperkeratosis and horny accumulation of keratinized material around the nails were peculiar findings in our case. Response to antitubercular treatment was excellent in our patient. Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10046f2.jpg] [dv10046f1.jpg] |
| |||||||||

{kind=link}
{kind=link}