 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
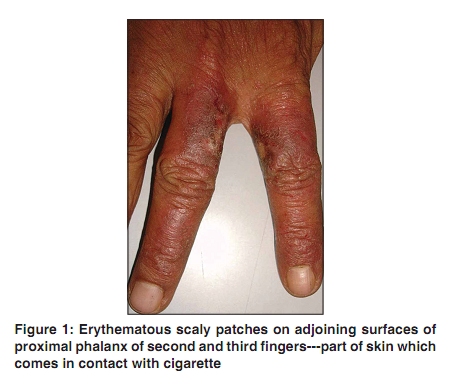
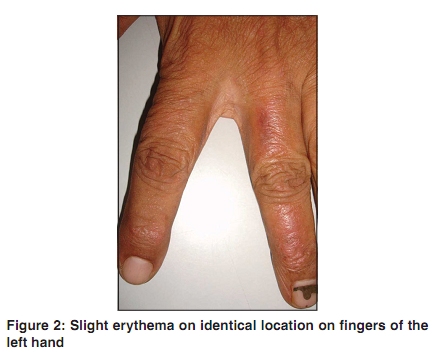
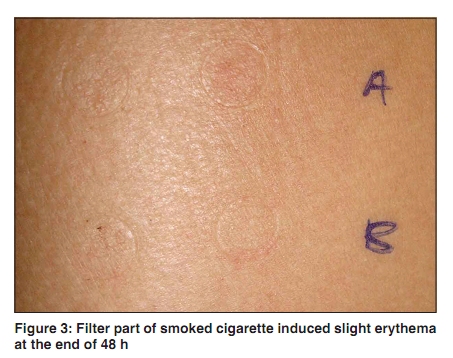
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 189-191 Letter to the Editor Non-occupational contact dermatitis to cigarette Prashant K. Palwade Keshav Skin and Hair Clinic and Dr Hedgewar Rugnalaya, Aurangabad, Maharashtra, India Correspondence Address: Dr. Prashant K. Palwade, Keshav Skin and Hair Clinic, Mahesh Nagar, Opposite St Francis School, Jalna Road, Aurangabad, Maharashtra - 431 003, India, drprashantpalwade@yahoo.co.in Code Number: dv10052 PMID: 20228556 DOI: 10.4103/0378-6323.60560 Sir, Hand dermatitis is common in dermatology practice, but it is quite uncommon to find an allergen responsible for it, even though one has a good contact dermatitis investigation and diagnosis set up. Hence, it becomes very important for a clinician to spare some time getting a detailed history so as to shortlist some of the possible allergens in patient day-to-day life. Cigarette smoking is a common habit and an addiction. Cigarettes are known to contain potent carcinogens and their smoke contributes to many chronic and potentially fatal diseases. Cigarette-induced allergic contact dermatitis (ACD) is uncommon. The following case, therefore, seems worthy of description. A 67-year-old-male presented with pruritic, red, scaly patches on second and third finger of right hand since a couple of months. On examination, erythematous scaly patches of size around 2 cm ´ 2 cm were seen on adjoining surfaces of proximal phalanx of second and third fingers [Figure - 1]; slight erythema was also noted on an identical location on fingers of the left hand [Figure - 2] All the possible causes of hand dermatitis were looked for and then a factor too often missed in dermatology history taking was enquired about, i.e. habits and addictions. He was a chronic cigarette smoker. While smoking he used to hold cigarette between second and third fingers of the right hand and sometimes in the left hand. He was using filter cigarettes of a specific brand since 30 years. He did not have lesions on lips or any other areas such as nose and cheeks, which are likely to be involved in cigarette dermatitis. Indian standard patch test series (CODFI) and an additional patch test to check which of the cigarette constituents were responsible for ACD were done. Unsmoked tobacco, smoked tobacco, smoked filter, and filter paper were used ′as is′ with white soft paraffin under aluminum discs (Finn chambers). At the end of 48 h, filter part of smoked cigarette induced palpable erythema [Figure - 3]. Standard patch test series was incidentally positive for neosporin. On enquiry it was found that he was using neosporin powder on ACD lesions on his finger. After a week, there was no delayed reaction to any of the tested allergens. Thus, clinical diagnosis of allergic contact dermatitis to cigarette filter and neosporin was confirmed. His skin lesions improved with topical momatasone furoate 0.1% ointment and a moisturizing cream. He was advised to discontinue his addiction for cigarettes so as to reduce the chances of recurrence of ACD and to live a healthy life. He was not ready to quit his addiction, so he was advised to wrap a paper around filter as a precaution to prevent ACD. Health hazards of cigarette smoking are numerous. Contact dermatitis from tobacco has mainly been described as an occupational cause of ACD. [1],[2],[3],[4],[5] It involves agricultural workers and those engaged in manufacturing or selling tobacco products, all of whom are in direct contact with tobacco and its products. ACD from tobacco may have been due to chemicals added during the plant cultivation and processing. [5] For example, patch-testing tobacco workers with moist processed tobacco leaves resulted in more positive reactions than did patch-testing with dried unprocessed leaves, and the potential allergens are waxes, paraffins, fatty acids, organic acids, aldehydes, ketones, phenols, paraphenols, catechols, and tannins. [5] There are very few reports in the literature exploring these allergens. ACD from cigarettes may clinically manifest itself as dermatitis on the fingers and mouth or as erythematous macules or pigmentation (or both) on the upper lip. [1],[2],[3],[4] Treatment of ACD to cigarette involves use of topical corticosteroids to reduce acute symptoms. But the most important part is to counsel patient about the best treatment strategy---quit smoking. If patient agrees well and good, if he/she does not, then possible ways to avoid contact with the cigarette and its components should be discussed. In spite of various campaigns by different authorities against tobacco and its products, cigarette smoking remains a common habit and an addiction. We as dermatologists should always look into this aspect of patient′s life style in suspected cases of allergic contact dermatitis and consider patch testing them with cigarette constituents in addition to standard patch test series. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10052f3.jpg] [dv10052f1.jpg] [dv10052f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}