 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
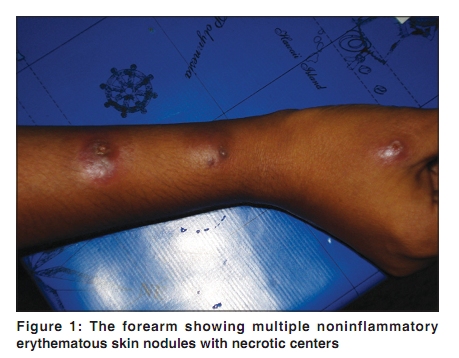
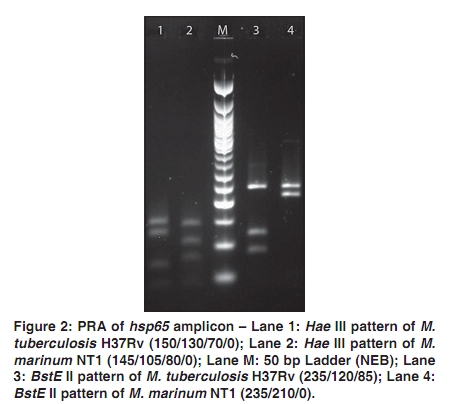
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 191-192 Letter to the Editor Do Mycobacterium marinum infections occur in India? Kidangazhiyathmana Ajithkumar, G. K. Madhavilatha1, Bhageerathy Sulekha, Sylvain Godreuil2, A.K. Anilkumar1, K. Girija, Sathish Mundayoor4 Medical College Chest Hospital, Thrissur, 1Mycobacterium Research Group, Department of Molecular Microbiology, Rajiv Gandhi Center for Biotechnology, Trivandrum, India, 2CHRU Arnaud de Villeneuve, Laboratoire de Bactériologie–Virologie, France Correspondence Address: Dr. Ajithkumar Kidangazhiyathmana, Dermatology and Venereology, Medical College Chest Hospital, MG Kavu, Thrissur - 680 581, Kerala, India, ajisudha@gmail.com Code Number: dv10053 PMID: 20228557 DOI: 10.4103/0378-6323.60562 Sir, Mycobacterium marinum, a close relative of M. tuberculosis, is an atypical Mycobacterium found in both salt and fresh water. [1] It causes a tuberculosis-like disease in frogs, fish and other cold-blooded animals, and a peripheral granulomatous disease in humans. Infection occurs following skin trauma, and usually presents as a localized granuloma or sporotrichotic lymphangitis. [2] A 29-year-old female sought treatment for skin lesions giving a history of a rose thorn prick, 2 months prior to the initial skin lesion. Physical examination showed multiple noninflammatory erythematous skin nodules with necrotic centers on the forearm of the left hand [Figure - 1]. Histopathology examination of the nodule showed granulomas with areas of suppuration. Special stains did not reveal any evidence of AFB or fungal elements. There was nothing contributory in the investigations including blood sugar, RFT, LFT and chest X-ray. She was HIV-negative. Results of Gram stain and routine culture from biopsy of skin lesions in both blood agar and McConckey agar were negative. A smear from the walls of the necrotic center when stained for acid-fast bacilli revealed organisms consistent with mycobacteria. Subsequent subculture on Lowenstein-Jensen medium at 37ºC became positive after 3 weeks showing small, round, smooth colonies. Genomic DNA was isolated and subjected to PCR, restriction analysis and sequencing. Partial sequencing of the 16S rRNA gene and the 16S-23S internal transcribed spacer (ITS) region was carried out for species identification. Analysis of a 984 bp fragment towards the 5¢ end of the 16S rRNA gene and a 403 bp fragment of the 16S-23S ITS region showed 100% similarity to both M. marinum M (CP000854) and M. ulcerans Agy99 (CP000325). But sequencing and analysis of 437 bp fragment towards the 3¢ end of the 16S rRNA gene showed 100% similarity with M. marinum M (CP000854). Also, a 441 bp fragment of the hsp65 gene was amplified and subjected to PCR restriction analysis (PRA) and sequencing. The pattern generated by the restriction analysis of the hsp65 amplicon with BstE II and Hae III endonucleases [Figure - 2] was as that of M. marinum ( http://app.chuv.ch/prasite/index.html ). The BLAST analysis of this amplicon showed 100% identity to M. marinum M (CP000854). Newly determined sequences of the isolate were deposited in GenBank (FJ868212, FJ868213, FJ868214 and FJ868215). Later, a commercial multiplex line probe assay, GenoType Mycobacterium AS/CM conclusively confirmed that it was indeed Mycobacterium marinum. PCR was also carried out to amplify the 549 bp sequence of the repetitive element IS2404 and no amplicon was obtained. This patient was treated with a combination of amikacin 750 mgm daily (15 mg/kg) and clarithromycin 500 mg twice daily with which lesions subsided over a six-week period with regular monitoring of renal function. A minor relapse after four weeks of treatment was managed with a further course of same treatment for another two weeks resulting in complete resolution of lesions. Nontuberculous mycobacteria (NTM) have had a strong impact on human populations in both developing and industrialized countries. [3] Their significance has increased after the onset of the AIDS epidemic, but the rate of nonAIDS-associated NTM infections is also increasing. [4] Specifically, disease caused by M. ulcerans, M. marinum, and M. haemophilum has increased in both healthy and immunocompromised patients in the last decade and moreover, these diseases have been reported from previously unaffected geographic areas, which indicate an increase in the geographic distribution of these organisms. Cutaneous infections by nontuberculous mycobacteria (NTM) are not usual but their relative importance has changed during the last few years and still further changes are expected. Mycobacterium marinum infection of humans, typically occurs when the bacterium is inoculated through the skin by cuts and scratches following direct contact with an infected fish or contaminated aquatic environments. [5] In our patient there was no definite history of contact with fishes but gave a history of rose thorn prick and also, the lesions presented were multiple erythematous skin nodules with necrotic centers on the forearm. The patient had never traveled outside India nor had come into close contact with travelers. To the best of our knowledge, this is the first conclusive report of M. marinum infection from India and also probably from the Indian Subcontinent. This implies that though M. marinum is present in the environment, either it had not caused infection till now or the infection had gone undetected. Thus improvements in diagnostic methods and closer collaborations between hospitals and research institutions would aid in the diagnosis of infections whose origin is unclear. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10053f2.jpg] [dv10053f1.jpg] |
| |||||||||

{kind=link}
{kind=link}