 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
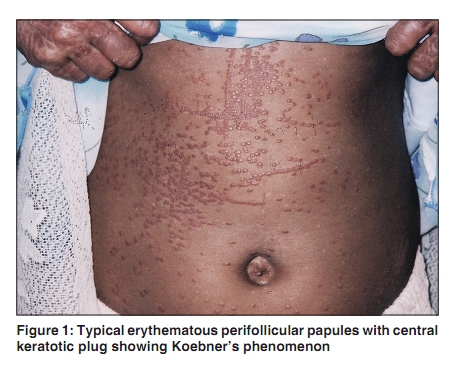
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 194-196 Letter to the Editor Pityriasis rubra pilaris with Koebner's isomorphic phenomenon Jayanta K Das, Asok Kr Gangopadhyay, Sujata Sengupta1 Department of Dermatology, Ramakrishna Mission Seva Pratisthan, VIMS, 99, Sarat Bose Road, Kolkata 700 026, W. B, India, 1B P Poddar Hospital and Medical Research Centre, New Alipore Block-G, Kolkata 700053, West. Bengal, India Correspondence Address: Dr. Sujata Sengupta, 9RB, Greenwood Nook. 369/2, Purbachal Kalitala Rd. Kolkata-700 078, India, senguptasujata@yahoo.co.in Code Number: dv10055 PMID: 20228559 DOI: 10.4103/0378-6323.60564 Sir, Pityriasis Rubra Pilaris (PRP) is a heterogeneous group of disorders showing circumscribed follicular keratoses, branny scale, orange-red erythema, and palmoplantar keratoderma. [1] In addition to the well-accepted five types, designated as type I to type V, type VI, has been suggested as occurring in patients with HIV infection. [1] The onset of juvenile onset classical (Type III) PRP is between the ages of 5 to 10 years. It often follows an acute infection. Spontaneous clearing is common within 1-2 years. [1] The isomorphic response of Koebner, named after Heinrich Koebner (1838-1904), is a well-known phenomenon commonly associated with psoriasis. [2] It has also been described in conjunction with a host of other disorders. [3] It involves the development of lesions in previously normal skin that has been traumatized either externally or internally. A seven-year-old girl presented with the history of erythematous scaly and slightly itchy eruption all over the body that started about a month back on the scalp. She gave no history of fever or any acute infection preceding the skin disease. Cutaneous examination on the first visit showed numerous lesions, each consisting of erythematous perifollicular papules with a central keratotic acuminate plug, on the upper chest, upper back, neck, shoulders, and dorsum of hands and feet. Face was uniformly erythematous with mild ectropion. Scalp showed diffuse bran-like scaling. Palms and soles were hyperkeratotic. Nails were thickened. On the second visit, after two weeks, the clinical condition had worsened. The most notable new finding was the typical erythematous perifollicular papules with central keratotic plug in linear distribution on the chest and abdomen. [Figure - 1] They were seen along a few almost straight lines coursing through the right lateral border and the lower border of the main group of erythematous perifollicular papules. On detailed questioning, it was learnt that about 10-12 days ago the patient suffered from injury by the sharp tip of a stick while playing. The trauma caused oozing of very little blood, and was on the chest and abdomen just along the lines where the new lesions in linear distribution came up later. Histopathology of skin biopsy sample taken from a typical lesion on the dorsum of the right hand showed features of PRP, such as acanthosis, and a follicle filled with dense, horny plugs, with a few parakeratotic cells in the perifollicular shoulder and in other parts of the epidermis, alternating with orthokeratotic epidermis. There was a mild mononuclear infiltrate in the dermis. Skin biopsy sample taken from a lesion on the abdomen induced by trauma showed histopathological picture similar to that of the hand lesion. Koebner phenomenon has been described in association with a lot of diseases; so the need for more stringent criteria for defining the isomorphic phenomenon has been stressed. [3] Boyd has proposed to ′reserve the isomorphic phenomenon solely for those diseases in which the phenomenon is reproducible in all manner of patients, by a variety of insults, and not due to dispersement (sic) of external infective or allergic element.′ [4] It is difficult to agree with his contention that the phenomenon must be reproducible in all manner of patients, for it is a well-known fact that even in psoriasis, lichen planus, or vitiligo, the three diseases showing uncontestable Koebner phenomenon, not all patients show the phenomenon, however hard they might be prodded. In his otherwise excellent review, Boyd has classified the reported Koebner Responses in four categories: [3],[4]
Boyd categorized Koebner phenomenon in PRP in class 4, i.e., as ′Poor or questionable trauma-induced process′ [4] For this particular disease Boyd mentioned an article by Farber et al. as his only reference. [4],[5] However, the Farber et al. study deals only with isomorphic response of Koebner in psoriasis, without mentioning Koebner phenomenon in PRP anywhere at all in his text. In the ′Discussion′ appended at the end of Farber′s article, Dr. Rees B. Rees commented, inter alia, that Koebner phenomenon occurs in PRP too; but Dr. Rees never cited any reference to substantiate his assertion. On the other hand, extensive search of the ′Pub med′ and ′Medline′ by us failed to yield any article documenting Koebner phenomenon in PRP. The large series by Clayton et al. also fails to record Koebner phenomenon in PRP. [6] In our case, previously normal skin was traumatized externally, and the exact site, time and type of trauma could be recorded and this was duly followed by development of characteristic lesions of PRP. As inducing Koebner phenomenon experimentally raises a lot of ethical questions, we have not tried that. Our case is possibly the first reported case of PRP showing almost uncontestable Koebner phenomenon, occurring in a case of type III, i.e., juvenile onset, classical PRP. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10055f1.jpg] |
| |||||||||

{kind=link}