 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
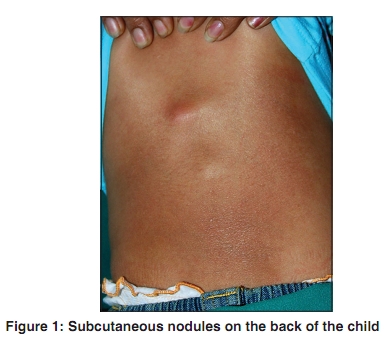
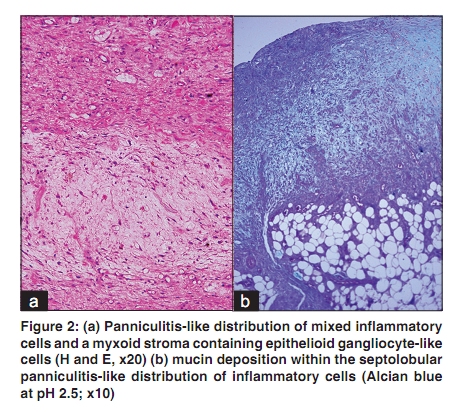
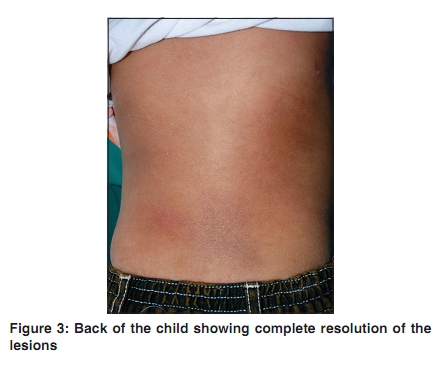
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 198-199 Letter to the Editor Self-healing juvenile cutaneous mucinosis manifesting with subcutaneous nodules Arti Nanda, Mohamed K Selim, Humoud Al-Sabah, Vivek Singhal1, Kusum Kapila2 As'ad Al-Hamad Dermatology Center, Al-Sabah Hospital, 1Department of Dermatology Yiaco Appollo Hospital, and 2Department of Pathology, Faculty of Medicine, Kuwait University, Kuwait Correspondence Address: Dr. Arti Nanda, P.O. Box: 6759, Salmiya, 22078, Salmiya, Kuwait, artinanda@hotmail.com Code Number: dv10057 PMID: 20228561 DOI: 10.4103/0378-6323.60567 Sir, Self-healing juvenile cutaneous mucinosis (SHJCM) is characterized by a rapid onset of papules, plaques, or nodules on the face, periarticular region, abdomen, and thighs. Lesions are associated with absent-to-mild inflammatory symptoms and in most cases show spontaneous complete resolution in weeks to months. Since its first report in 1973, [1] around 15 cases have been reported in the literature. [2],[3],[4],[5] The exact pathogenesis of SHJCM is not clear. We report an additional case of SHJCM in a two and a half years old female child, who presented with subcutaneous nodules clinically with histopathological changes affecting the subcutaneous tissue. A two and a half years old girl presented with progressive asymptomatic nodules preceded by minor trauma on the face and scalp, followed by similar lesions on the neck, forearms, wrists, and back of 6-months duration. She was delivered at 34 weeks by normal vaginal delivery with a birth weight of 1.2 kg. Antenatal history of the mother and family history were unremarkable. There was no history of accompanying constitutional or systemic symptoms. Her physical and mental development was appropriate for her age. On examination, her height and weight were at 50th percentile. She was observed to have around 12 subcutaneous, mildly erythematous, firm, non-tender nodules up to 5 cm in diameter present on scalp, forehead, cheeks, neck, forearms, wrists, knuckle areas, and back [Figure - 1]. An excision biopsy was performed of two of the nodules, one on left forearm and another on the scalp. The biopsy specimens of both nodules stained with hematoxylin-eosin stain revealed a normal epidermis, and an unencapsulated deep dermal and subcutaneous mass composed of septolobular panniculitis-like distribution of mixed inflammatory cells within a myxoid stroma. Multiple epithelioid gangliocyte-like cells within the pool of myxoid stroma were seen [Figure - 2]a. The section stained with alcian blue at pH 2.5 confirmed the mucin deposition [Figure - 2]b. Various other investigations including complete blood counts, serum biochemistry, antinuclear antibodies, urinalysis, and X-ray of the skull were normal. On follow-up, 2-months later the lesions were observed to regress in size. At 5-month follow-up, all the lesions had resolved without any residual effect [Figure - 3]. One year later, after the regression of all the lesions, she continues to be in a good general health without any recurrence of lesions. SHJCM is a distinct variant of primary cutaneous mucinosis that can be differentiated from other variants of primary cutaneous mucinosis by a younger age of onset, rapid appearance of papules and/or nodules that tend to show spontaneous resolution. Nagaraj and colleagues [2] recently described the clinicopathological characteristics of three cases of SHJCM and reviewed the literature on 10 previously reported cases of SHJCM. The ages of the patients reported have ranged from 13 months to 15 years. Clinically, the skin lesions in SHJCM are of three types and include translucent to ivory white, grouped papules; deep-seated nodules; and periorbital or zygomatic edema. The striking feature is the self-healing nature of the lesions within weeks to months. Our patient is the classical example of nodular variant of SHJCM. A skin biopsy of the nodular lesions like our patient may show the diffuse septolobular panniculitis pattern with mucin deposition and the presence of epithelioid gangliocyte-like giant cells in myxoid stroma. Histologically, such cases may need to be differentiated from panniculitis, proliferative fasciitis, and other entities where gangliocyte-like giant cells are noted. [2] The clinical presentation with self-healing nature of skin lesions and mucin deposition in papillary and reticular dermis and presence of gangliocyte-like giant cells within the myxoid stroma help to differentiate SHJCM from proliferative fasciitis and other types of panniculitis. In contrast to mucinosis affecting adults, SHJCM runs a benign course and is not associated with disorders such as paraproteinemia, bone marrow plasmacytosis, or thyroid disorder. However, incidental associations with systemic lupus erythematous; fever and arthralgias; nephroblastoma; and bilateral carpel tunnel syndrome have been reported. [2],[3],[4],[5] None of these conditions were present in our patient. The etiopathogenesis of SHJCM is not settled. Abnormal fibroblast proliferation and mucin production are postulated to be secondary to a reactive or reparative response to a chronic antigenic stimulation, such as viral infection or inflammation. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10057f2.jpg] [dv10057f3.jpg] [dv10057f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}