 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
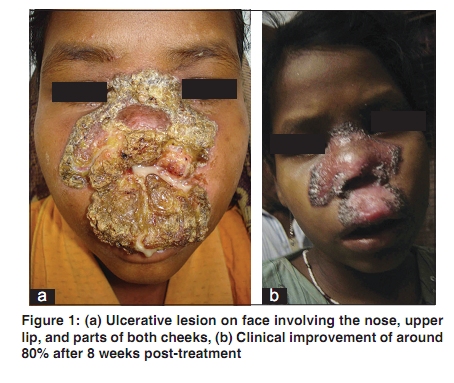
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 199-200 Letter to the Editor Mutilating lupus vulgaris of face: An uncommon presentation Binodini Behera, Basanti Devi, Nibedita Patra Department of Dermatology, Venereology and Leprology, S.C.B Medical College, Cuttack - 753 007, Orissa, India Correspondence Address: Dr. Binodini Behera, Department of Skin and VD, S.C.B. Medical College, 3R/9, Cancer wing, S.C.B. Medical College, Cuttack - 753 007, Orissa, India, drbinodini@gmail.com Code Number: dv10058 PMID: 20228562 DOI: 10.4103/0378-6323.60568 Sir, Lupus vulgaris is a chronic and progressive form of cutaneous tuberculosis occurring in individuals of moderate immunity and high degree of tuberculin sensitivity. It is the most common type with the most varied manifestations. [1] Face is most commonly affected in European countries. [1] In India, the buttocks, thighs, and legs are more common sites of involvement. [2],[3] A 13-year-old girl presented with a 2-year history of single ulcerative lesion on the face involving the nose, upper lip and some parts of both cheeks [Figure - 1]a. It started as a small papule, which broke down to form an ulcer on the tip of the nose. The ulcer gradually extended to both cheeks and the upper lip. There was no history of cough, weight loss, fever, or chronic diarrhea. No hoarseness of voice was found clinically. No history of tuberculosis in family or neighborhood was found. On examination an ulcerated, crusted plaque of size 10 x 8 cm was present over nose, malar area and upper lip. There was mucopurulent discharge from the ulcer and the nasal apertures were almost obliterated. The mucous membrane of upper lip and nasal mucosa were also involved with enlarged and mildly tender submandibular lymph nodes. Hematological and biochemical investigations were within normal limits, except relative lymphocytosis. ESR was 92 mm in first h, and the Mantoux test was positive with an induration of 24 mm transversely across the forearm. X-ray of the chest was normal. X-ray of paranasal sinuses showed features of chronic sinusitis. VDRL and ELISA tests for HIV were negative. Pus for culture and sensitivity showed growth of Staphylococcus aureus. Histopathological examination from the edge of the lesion showed granulomatous lesions with diffuse lymphocytic infiltration and multinucleated Langhan′s giant cells. The patient was given a course of oral antibiotics and was started with the standard anti-tuberculosis therapy [Category 3 under DOTS therapy- isoniazid (600), rifampicin (450), pyrazinamide (1500)] three times a week in the intensive phase simultaneously. The mucopurulent discharge subsided within 5 days, and the lesion started showing signs of healing at the center within 2 weeks. After 8 weeks of treatment, the lesion showed healing of up to 80 % [Figure - 1]b. The earliest description of lupus vulgaris was given by Erasmus Wilson in 1865, which compared the lesions to ravages of a wolf. [4] It usually starts as a soft brownish red papule or nodule that gradually expands by involution in one area with expansion in another, and sites of atrophic scarring are characteristic. Involvement of the nasal or auricular cartilage causes extensive destruction and disfigurement. In Western countries, the frequent localization of the lesions around the nose and on the cheeks is attributed to the rich and porous venous plexus with stasis, cold and hypoxia and impaired fibrinolysis and host defense at a lower temperature. [4] However, in India the higher temperatures prevailing in most parts may be responsible for relatively a low frequency of the facial lesions. As the involvement of nose with lupus vulgaris is quite uncommon in India, it often remains undiagnosed or misdiagnosed and leads to various mutilating and irreversible deformities of the face as for example in our patient who suffered for last 2 years. This delay in diagnosis and the facial deformity could have been averted by a high index of clinical suspicion and simple histological examination with proper commencement of therapy done early in the course. Also in a developing country like ours where the prevalence of tuberculosis is so high, it should be kept as a differential diagnosis in mind wherever indicated. The clinical differential diagnosis of lupus vulgaris involving the nose includes various infective and non-infective disorders showing a predilection for nose and adjoining areas of face such as leishmaniasis, rhinoscleroma, Wegener′s granulomatosis, sarcoidosis, etc. The present case is being reported because the ulcerative mutilating variety of lupus vulgaris in face has been sporadically reported from India. Three cases have been reported earlier to the best of our knowledge.[5],[6],[7] Our case although had healing of the lesion, she may require plastic surgery later due to resultant ugly deformity and scar which could have been avoided by early diagnosis and treatment. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10058f1.jpg] |
| |||||||||


{kind=link}