 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
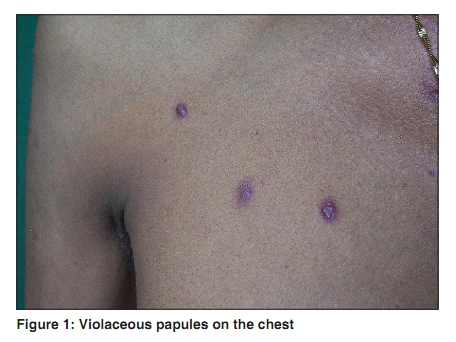
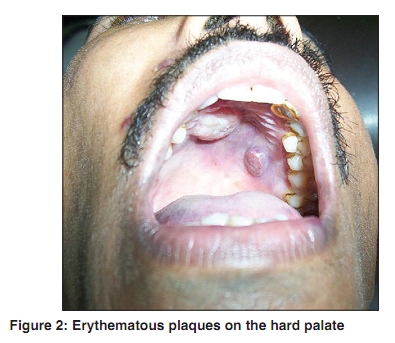
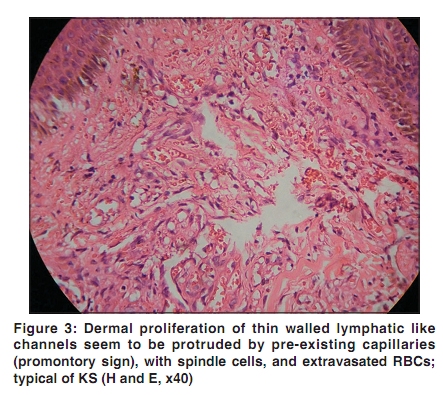
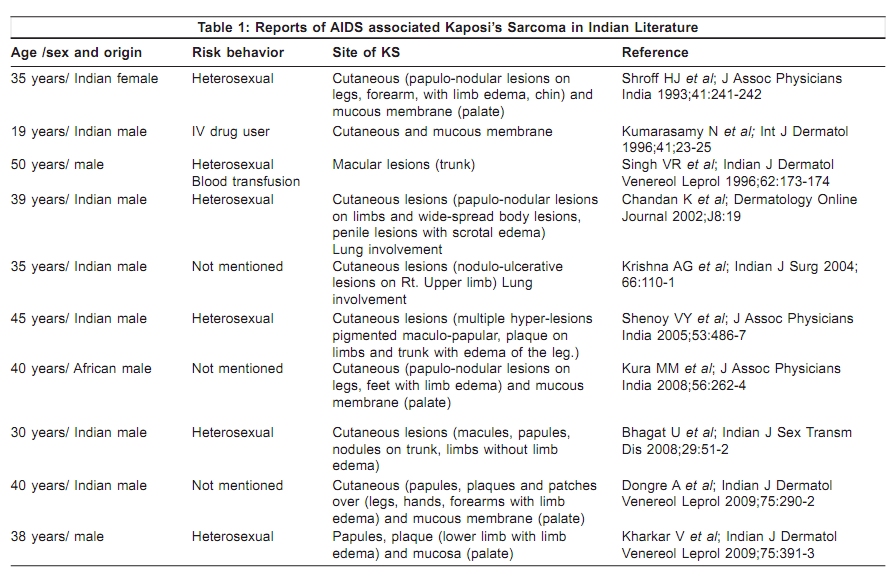
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 215 Net Case Kaposi's sarcoma: A presenting sign of HIV Jignesh B. Vaishnani, Sanjay S. Bosamiya, Anjum M. Momin Surat Municipal Institute of Medical, Education & Research (SMIMER), Umarwada, Surat - 395 009, Gujarat, India Correspondence Address: Dr. Sanjay S. Bosamiya, Department of Dermatology, Surat Municipal Institute of Medical Education & Research (SMIMER), Umarwada, Surat - 395 009, Gujarat, India, drsanjay_bosamiya@yahoo.co.in Code Number: dv10062 PMID: 20228569 DOI: 10.4103/0378-6323.60542 Abstract Kaposi's sarcoma (KS) is a multifocal cutaneous and extra cutaneous vascular proliferative disorder. In India, there are only a few cases of HIV-associated KS in published literature. A 26-year-old married man presented with asymptomatic elevated skin lesions over the face, trunk, both upper limbs and lower limbs with a duration of one-and-a-half months. Cutaneous examination revealed multiple violaceous papules and nodules, on the face (right upper and lower eyelids, upper lip), trunk and proximal part of both limbs. Oral cavity showed erythematous plaques, two in number, on the hard palate. Skin biopsy showed proliferation of thin walled capillaries with formation of slit like spaces, spindle cell proliferation, abundant extravasation of RBCs and moderately dense inflammatory infiltrate in the dermis. Thus a clinical diagnosis of cutaneous KS was confirmed. On testing with ELISA for HIV, the patient was for the first time diagnosed as HIV reactive. Thus KS was the presenting manifestation of HIV disease.Keywords: Kaposi′s sarcoma, HIV, India Introduction Kaposi′s sarcoma (KS) is a multifocal vascular proliferative disorder with some characteristics of neoplasm, but may involute spontaneously with improvement in the host′s immune function. HIV-associated KS displays a variety of distinct clinical features, which may differ considerably from those seen in other forms of the disease. Case Report A 26-year-old married man presented with asymptomatic elevated skin lesions over the face, trunk, both upper limbs and lower limbs, with a duration of one and a half months. Patient had a history of recurrent fever and weight loss for the last six months and diarrhea for the last two months. He had been treated for it by local doctors, but with only symptomatic improvement. There was no history of hemoptysis, hematemesis or melena. Patient had history of multiple heterosexual exposures, and denied any homosexual exposure. There was no history of intravenous drug abuse or blood transfusion. Lesions started on the face and gradually spread to involve the trunk, both upper limbs and lower limbs over a period of one-and-a-half months. Lesions were initially small, reddish and flat, and then gradually enlarged to become violaceous and elevated. Patient′s look was cachectic. Cutaneous examination revealed multiple violaceous papules and nodules, on the face (right upper and lower eyelids, upper lip), trunk [Figure - 1] and proximal part of both limbs. Lesions of molluscum contagiosum were present on the face with koebnerization. Oral cavity showed erythematous plaques, two in number on the hard palate [Figure - 2]. There was no lymphadenopathy and hepatosplenomegaly. With a clinical differential diagnosis of KS and bacillary angiomatosis, we referred him to the Integrated Counseling and Testing Centre (ICTC) for HIV testing, and he was, for the first time, diagnosed as HIV reactive. We took the biopsy from a papule over the back and until we received the biopsy report, we put him on a therapeutic trial of erythromycin for bacillary angiomatosis, which turned out to be unsuccessful. His absolute CD4+ count was 186 cells/mm 3 . Other laboratory investigations revealed a hemoglobin of 8.8 gm/dl, total white blood cell count of 7000 cells/mm 3 and a differential count of polymorphs-77%, lymphocytes-20%, monocytes-2%, eosinophils-1%. Liver and renal function tests were normal. Serology for HBsAg and VDRL was negative. X ray chest was normal. Sputum for Acid Fast Bacilli was negative. Chest and abdominal computerized tomography scan was done to rule out systemic involvement. His skin biopsy [Figure - 3] report revealed proliferation of thin walled capillaries, along the blood vessels of superficial plexus. The capillaries were arranged in a clustered pattern and could be seen as rounded spaces filled with red blood cells (RBCs) or slit like spaces, which extend between the collagen bundles formed by the proliferation of spindle cells arranged in short fasicles. Moderately dense infiltrate of lymphocytes and occasional neutrophils were present in the dermis. Abundant extravasation of RBCs was seen in upper dermis along with some hemosiderin deposits. Thus a clinical diagnosis of cutaneous KS was confirmed. Immunohistochemistry for CD31, CD34 and anti-LANA (antibodies to latency antinuclear antigens) for HHV-8 could not be done because of lack of facility in our set up. Discussion KS was initially described by the Hungarian dermatologist, Morris Kaposi in 1872. There are four recognized clinical subsets of KS- Classical, Endemic (African), KS associated with non-HIV induced immunosuppression and with HIV infection (epidemic). HIV- associated KS was first recognized in 1979 when an epidemic of KS was identified in the homosexual community in New York. [1] The World Health Organization (WHO) clinical staging for HIV/AIDS recognizes KS as an AIDS-defining illness. HIV-associated KS is common among homosexual men; it is uncommon in countries where HIV is predominantly transmitted heterosexually. Because of this, despite high prevalence of HIV/AIDS in India, only 10 cases of KS exist in the published literature [Table - 1]. This low prevalence of KS may be attributed to the low prevalence of HHV-8 in our country. [2] HIV-associated KS is usually asymptomatic, may be seen at any stage of HIV infection, even at normal CD4+ count [3] and CD4+ count is not a consistent prognostic indicator. In contrast to the other variants of KS, HIV associated KS can appear on any part of body with initial lesions frequently developing on the face, especially on the nose, eyelids, and ears-and on the trunk. Lesions of KS usually start as macule, progress to form papule, plaque and nodule. Sometimes pronounced lymphedema is observed in association with KS on the extremities, scrotum, penis, and face, especially when the eyelids are affected. Unusual cutaneous forms of KS include presentation like lichen planus, thrombophlebitic, telangiectatic, ecchymotic, pyogenic granuloma, indurated plaque, keloidal, warty exophytic, and lymphangiomatous. [4] The lesions of AIDS-related KS, frequently involve the mucous membrane, lung, lymph node, and gastrointestinal tract. [5] The oral mucosa is the initial site of localization in 10-20% of all HIV-associated KS and is frequently located on the palate. Diagnosis of cutaneous KS is made on clinical ground and confirmed by histopathological examination. Prognosis of epidemic KS is related to the extent of KS, underlying immunosuppression, opportunistic infections, and treatment of HIV infection. [6] An excellent staging system has been developed by the National Institute of Allergy and Infectious Disease AIDS clinical trials group (ACTG). It distinguishes patients on the basis of tumor extent, immunological function and the presence or absence of systemic disease. [7] Good prognosis is expected when CD4 count is> 200/mm 3 , only cutaneous involvement seen and no "B" symptoms (fever, weight loss, diarrhea). The fundamental basis for the treatment of AIDS-related KS is the suppression of HIV replication by starting antiretroviral treatment and treating the opportunistic infection. HAART can significantly decrease the incidence of KS, slow the rate of progression of KS and even result in regression of the preexistent disease. [8] Local treatment modalities include cryotherapy, intralesional vinblastine or vincristine, laser and radiation therapy. It is useful when skin or mucosal lesions are few and there is no systemic involvement. Indications for systemic therapy include (1) visceral involvement, (2) extensive KS associated with lymphedema, (3) extensive and rapidly progressing KS and (4) failure to respond to local therapy. US FDA has approved liposomal anthracyclines (doxorubicin and daunorubicin) as the first line agent for KS. Paclitaxel appears to be more effective than liposomal anthracycline but because of the high toxicity paclitaxel is second line therapy. [9] Other systemic therapy includes interferon-alpha and a combination of chemotherapy. We report this case for its rarity in India and the occurrence of KS as the presenting manifestation of HIV disease. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10062f2.jpg] [dv10062f1.jpg] [dv10062f3.jpg] [dv10062t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}