 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
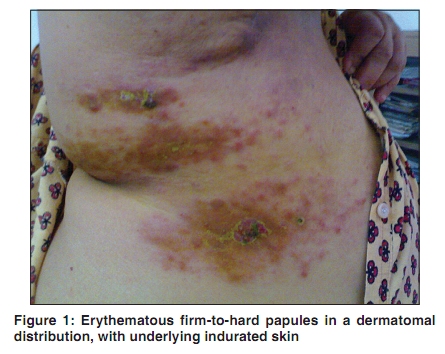
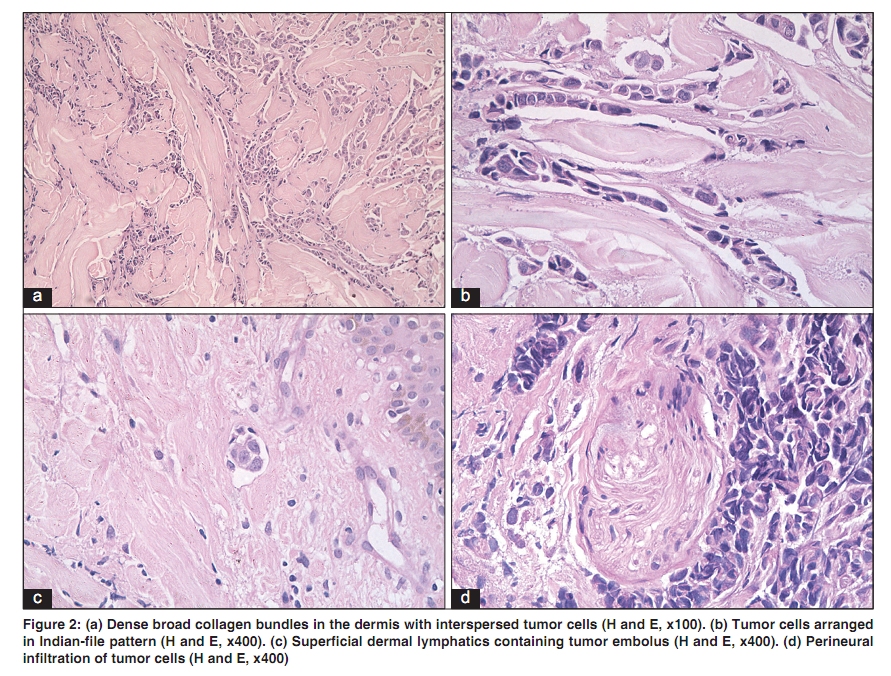
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 215 Net letter Carcinoma en cuirasse of the breast with zosteriform metastasis Chembolli Lakshmi, Suma B. Pillai1, Chetna Sharma1, C. R. Srinivas Department of Dermatology, 1Pathology, PSG Hospitals & PSGIMSR, Peelamedu, Coimbatore - 641 004, India Correspondence Address: Dr. Chembolli Lakshmi, Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore - 641 004, Tamil Nadu, India, cl_coimbatore@yahoo.co.in Code Number: dv10064 PMID: 20228567 DOI: 10.4103/0378-6323.60544 Sir, En cuirasse metastatic carcinoma is characterized by diffuse morphea-like induration of the skin. It is a fibrotic process resembling the encasement in an armor of a curassiere (cavalry soldier). [1],[2] It evolves from firm papules and nodules overlying an erythematous base to a sclerodermoid plaque. [3] Pain and pruritus may be the associated features, unlike cutaneous metastases, which usually present as asymptomatic, painless, firm or doughy skin-colored papules or nodules. Carcinoma en cuirasse in a dermatomal distribution has not been reported. A 62-year-old postmenopausal lady who had undergone mastectomy for adenocarcinoma of the right breast two months back, presented with painful erythematous lesions over the right side of her chest, of one-month duration. There were no palpable lymph nodes in both the axillae or palpable nodules in the opposite breast. Numerous firm-to-hard erythematous papules and few indurated coalescent plaques with superficial ulceration and crusting were present over the right side of the chest in a dermatomal distribution (spread over the dermatomes T5 - T7). The evolution of lesions was from a papule that coalesced in few areas to form an indurated plaque. The underlying skin was erythematous, woody hard, and unpinchable [Figure - 1]. There was a burning pain along the distribution of the lesions, which on closer examination were papules, although they gave the impression of being papulovesicular. Biopsy from a papule confirmed a metastatic adenocarcinomatous deposit. The dermis showed infiltration by tumor cells arranged in cords (Indian-file pattern) [Figure - 2]a and groups between the dense broad collagen bundles [Figure - 2]b. An occasional glandular pattern was also seen. Tumor emboli were seen in the superficial dermal lymphatics [Figure - 2]c. Perineural infiltration by tumor cells was also seen [Figure - 2]d. Cutaneous metastases from solid primary tumors are rare. Eight clinicohistopathological types of skin involvement are seen with metastatic breast cancer, which include carcinoma en cuirasse, inflammatory telangiectatic and nodular types of metastatic carcinoma, alopecia neoplastica, carcinoma of the inframammary crease, metastatic mammary carcinoma of the eyelid with histiocytoid histology, and Paget′s disease. [4] Targetoid metastasis has also been reported. [5] Carcinoma en cuirasse is characterized histologically by dense fibrosis and decreased vascularity, making it highly resistant to chemotherapy. Perineural invasion of the nerves could account for the burning pain associated with the lesions. The induration could be related to chronic lymphatic obstruction as proposed by Hanley. [6] Tumor emboli within the superficial lymphatics were seen in our patient. The mechanism for the zosteriform appearance of the metastatic disease is not known. It has been postulated to occur as a Koebner response to recent herpes zoster.[7] However, our patient did not report any skin lesions over the area prior to the development of the present lesions. Perineural lymphatic metastatic dissemination has also been suggested, [8] and is likely to be the cause of our patient having dermatomal distribution of skin lesions associated with burning pain. To our knowledge, carcinoma en cuirasse in a dermatomal distribution has not been reported. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10064f1.jpg] [dv10064f2.jpg] |
| |||||||||


{kind=link}
{kind=link}