 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
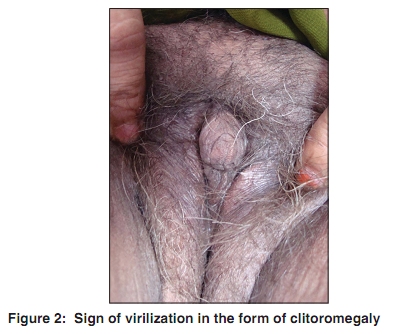
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 216 Net letter Hirsutism with virilization in a postmenopausal woman due to a rare ovarian steroid cell tumor Sanjiv V. Choudhary, Pankaj J. Banode1, Arvind Bhake2, Sankalp Dwivedi3, Sumit Gupta, Sankha Koley, Adarshlata Singh Departments of Dermatology, 1Radiology, 2Pathology and 3Surgery, Jawaharlal Nehru Medical College, Sawangi, India Correspondence Address: Dr. Sanjiv V. Choudhary, 28, Modern Nagpur Society, Chhatrapati Nagar, Nagpur-15 [MS], India, sanjiv_choudhary26@yahoo.com Code Number: dv10066 PMID: 20228571 DOI: 10.4103/0378-6323.60546 Sir, Hirsutism is defined as the occurrence in women and children of growth of coarse terminal hair in a male sexual pattern. These areas include the lips, chin, chest, abdomen, back, and femoral region, where normally very few hairs are found. Hirsutism can be induced by excessive endogenous androgen production either by the ovaries or by the adrenal glands, central over production of androgens, increased peripheral conversion of androgens, decreased metabolism, and enhanced receptor binding. Hyperandrogenemia is the key trigger for excess hair growth. Non-androgen-induced hirsutism can be idiopathic, familial, or drug induced. Ovarian steroid cell tumors are characterized by cells with abundant intracellular lipids that are similar to adrenocortical cells. They account for 0.1-0.2% of all ovarian tumors, and the majority of them show virilization. [1] There are three subtypes: stromal luteoma, Leydig cell tumor, and steroid cell tumor, not otherwise specified (NOS). Steroid cell tumor, not otherwise specified, accounts for approximately 60% of steroid cell tumors, 25-45% of which are clinically malignant. [1],[2] Half of the cases with this subtype are associated with androgenic changes. Tumors causing virilization are often small. [1],[3] The majority of steroid cell tumors have a benign or low-grade behavior. Interestingly, pathologically benign tumors can behave in a clinically malignant fashion. Steroid cell tumors often present as unilateral solid tumors and occasionally as cystic tumors. Steroid cell tumor (NOS) can occur at any age (mean, 42 years). A 50-year-old female patient, housewife, presented with excessive abnormal hair growth involving the face, chest, and thigh for 5 years. The hair growth was gradual to begin with but since 1 year, she noticed more rapid hair growth involving the face and chest region. The patient has attained her menopause. Symptoms of virilization were present in the form of deepening of voice and thinning of scalp hair. Cutaneous examination revealed thick dark terminal hairs involving the upper lip, chin, submandibular region [Figure - 1], chest, and anterior aspect of thigh. Signs of virilization were present in the form of clitoromegaly [Figure - 2], frontal baldness, loss of female body contours, increased muscularity, and atrophy of breast. Abdominal examination showed no abnormality and vaginal examination disclosed clitoromegaly. A thorough endocrinal work-up at an outside facility showed a grossly elevated serum testosterone concentration of 207 ng/dl and a free testosterone concentration of 50 pg/ml. A transvaginal ultrasonography (USG) revealed a 3.8 × 2.9 × 3.1 cm sized well-defined isoechoic lesion in the left ovary showing moderate intralesional vascularity. Additionally, computed tomography (CT) scan imaging was obtained, which confirmed the well-defined rounded soft tissue moderately enhancing mass in the left ovary. No significant regional lymphadenopathy was noted. USG-guided FNAC from the left ovary was done. The smear showed fragments of loosely adhered polygonal cells with vacuolated lipid-filled cytoplasm and round hyperchromatic centrally placed nuclei. The cytoplasm and margins are prominent. The background shows tiny lipid vacuoles mixed with hemorrhagic material. A preoperative diagnosis of testosterone-producing sex-cord stromal cell tumor of the left ovary was made. Considering the age of the patient, hysterectomy with bilateral salpingo-oophorectomy was done. Post-operative histopathological examination of the left ovary sections revealed features suggestive of lipid cell tumor in the form of many lipid containing vacuolated cells with central and eccentric hyperchromatic nuclei. The cytoplasm of few cells appeared granular and finely vacuolated. The stroma was thin and lipid filled. The right ovary showed follicular cyst. Myometrium revealed adenomyoma and cervix showed mild dysplasia with hypertrophied squamous epithelial lining. The serum levels of testosterone returned to normal immediately after the surgery. Androgen-secreting ovarian tumors are rare but may be seen later in life. They are Sertoli-Leydig cell tumors, granulosa-theca cell tumors, and lipid cell tumors. Hayes and Scully [4] reported 63 cases of ovarian steroid cell tumors ranging from 2 to 80 years of age. Steroid cell tumor, NOS, is a rare ovarian tumor (0.1%) and the average age of occurrence is at 43 years. [5] In our case, the clinical signs and symptoms indicative of hyperandrogenemia started around the age of 45 years. At that time, the patient had attained her menopause. Steroid cell tumors of the ovary have interesting presentations related to the hormonal activity and virilizing properties of the tumor. Reedy et al. reported a case of an undifferentiated NOS steroid cell tumor with hirsutism, amenorrhea, clitoromegaly, and temporal baldness. [6] In our case, hirsutism was associated with signs of virilization in the form of deepening of voice, clitoromegaly, frontal baldness, and increased muscularity. In androgen-secreting ovarian tumors serum testosterone levels are often high, but DHEA-sulfate levels are low. Our patient also had grossly elevated serum testosterone but normal DHEA-sulfate levels. Differential diagnosis of steroid cell tumor includes luteinized granulosa cell tumor, thecoma, clear cell carcinoma, metastatic renal cell carcinoma, and lipid-rich sertoli cell tumor. [5] All these were excluded before reaching our diagnosis of steroid cell tumor, NOS. The diagnosis of these rare tumors can be problematic especially in the case of a small nonpalpable ovarian tumor. Vaginal ultrasonography has been successfully used to detect ovarian pathologies. In our case, transvaginal pelvic ultrasonography revealed a small well-defined isoechoic lesion, which was clinically nonpalpable, in the left ovary and was also confirmed by CT scan findings. Our patient underwent hysterectomy with bilateral salpingo-oophorectomy. We made the final diagnosis of a rare ovarian steroid cell tumor by histopathological examination of the surgically resected material. We report this case for its rarity and its classical presentation. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10066f1.jpg] [dv10066f2.jpg] |
| |||||||||

{kind=link}
{kind=link}