 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
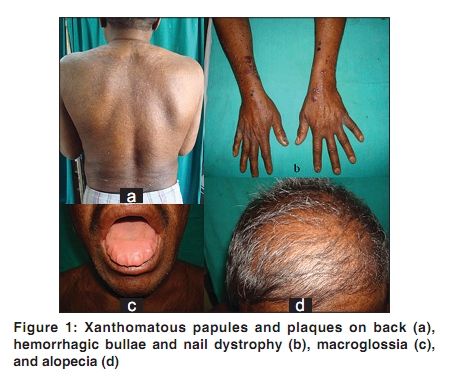
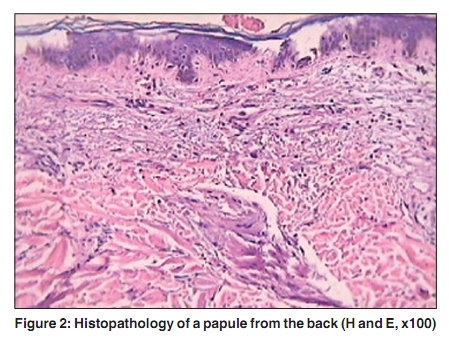
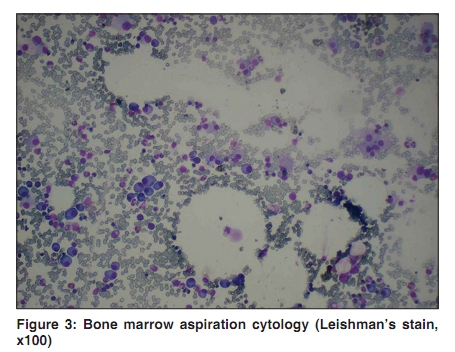
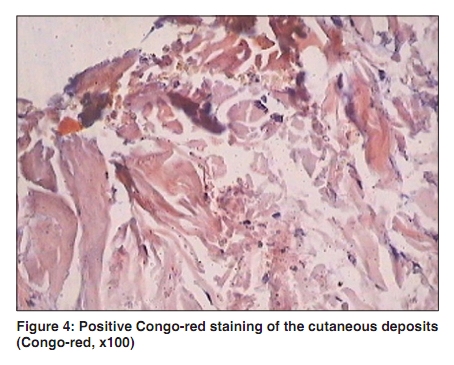
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 2, March-April, 2010, pp. 216 Net Quiz Fatigue, macroglossia, xanthomatous papules and bullae Sanjay Singh, Surendra Kumar, Rahul Chaudhary Department of Dermatology, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, India Correspondence Address: Dr. Sanjay Singh, C-9 New Medical Enclave, Banaras Hindu University, Varanasi - 221 005, India, sanjaye2@gmail.com Code Number: dv10067 PMID: 20228570 DOI: 10.4103/0378-6323.60547 A 45-year-old man had fatigue, nail dystrophy (thinning, striations) (13 months); diffuse scalp alopecia, macroglossia, dysphagia (4 months); xanthomatous lesions, hoarseness, generalized pruritus (3 months); and bullae (6 weeks). Except pallor and expressionless face, general and systemic examination was normal. Itchy, xanthomatous papules were present on the back [Figure - 1], and tense vesicles and bullae, some with hemorrhagic fluid, were on the limbs and abdomen. Hemoglobin was 7.8 g/dl, and ESR was 31 mm. Blood counts, routine urinalysis, and serum biochemistry including calcium level, X-rays and ultrasonography (abdomen) were normal. The 24-h urinary protein was 360 mg/dl. Skin biopsy [Figure - 2] and bone-marrow examination [Figure - 3] were performed. What is Your Diagnosis ? Diagnosis: Systemic amyloidosis Pinching a papule in the axilla produced purpura. Histopathology of a papule showed thickened bundles of collagen, some showing uniformly pink-stained amorphous fissured material within them [Figure - 2]. The deposits were also present within the walls of the blood vessels (venules). There was no inflammatory infiltrate. Congo-red stain was positive [Figure - 4], diagnosing the deposits as amyloid. Bone-marrow cytology showed> 35% plasma cells consistent with multiple myeloma [Figure - 3]. Serum electrophoresis showed M-band, while urine electrophoresis showed Bence Jones proteinuria. Serum beta2 microglobulin was 3074 µg/dl. On the basis of these findings, a final diagnosis of multiple myeloma-associated systemic amyloidosis was made. Discussion Amyloidosis is caused by extracellular deposition of insoluble abnormal fibrils formed by the aggregation of misfolded, normally soluble proteins. [1] Types of amyloidosis include systemic AL amyloidosis (due to multiple myeloma or low-grade monoclonal gammopathy), reactive systemic AA amyloidosis (due to chronic inflammatory, infective or neoplastic diseases), hereditary amyloidosis, and localized amyloidosis. [2] AL amyloidosis is a plasma cell dyscrasia with immunoglobulin light chains or their fragments forming amyloid. [3] Upto 15% of patients with myeloma have amyloidosis. [2] Amyloid deposition can occur in any organ in AL amyloidosis, [3] most commonly in the kidneys or in the heart. [1] Presenting symptoms include fatigue, weight loss, paraesthesia, hoarseness and edema. Diagnostically useful presenting features are carpal tunnel syndrome, macroglossia, and mucocutaneous lesions. Mucocutaneous lesions occur in 30-40% of patients. [1] Most characteristic skin lesions are waxy-looking, yellowish, papules or plaques. Other important cutaneous manifestations are petechiae, purpura, and pinch purpura. Rare cutaneous manifestations include alopecia, nail dystrophy (whitening, banding, brittleness and onycholysis), [3] and scleroderma-like changes. [2] Tense bullae, often hemorrhagic, occur rarely in the skin [2] or in the mucous membranes. [3] Coarse facies (loss of wrinkles) result from infiltration. Multiple myeloma patients have generalized pruritus with unknown frequency. A skin biopsy shows amorphous, fissured eosinophilic masses in the dermis or subcutis. Characteristically amyloid deposition may occur in the blood vessel walls, pilosebaceous units, sweat glands, and around the fat cells in subcutis (amyloid rings). [1] Congo red staining differentiates amyloid from other hyaline deposits. [3] Cross-polarized light shows red-green dichroism. Immunohistochemistry yields definitive results in AA amyloidosis, but is frequently not diagnostic for AL deposits. [2] Prognosis of AL amyloidosis is poor (5-year survival approximately 10% and 10-year survival < 5%), usually because of late diagnosis. [2] Death usually results from cardiac or renal failure. Skin lesions may be early or even presenting features, providing an opportunity for early diagnosis. Intervention may then be initiated before end-organ failure and further disease progression may be delayed. The most important prognostic factor is the stage of the disease when initiating treatment, thus demonstrating paramount importance on early diagnosis. [3] Patients with AL amyloidosis were usually treated with oral melphalan and prednisone, but response is unsatisfactory and delayed. [4] Treatment of selected patients by high-dose melphalan and autologous stem-cell transplantation (ASCT) resulted in hematologic remission, improved 5-year survival, and reversal of amyloid-related disease in many patients. [5] Most efficient treatment for AL amyloidosis is ASCT; however, toxicity limits its feasibility to some patients only. [4] Melphalan and high-dose dexamethasone represents a feasible and effective treatment for patients with advanced AL amyloidosis ineligible for ASCT. [4] Furthermore, the novel therapies---thalidomide, bortezomib, and lenalidomide---have resulted in improved survival rates. [6] References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10067f2.jpg] [dv10067f4.jpg] [dv10067f3.jpg] [dv10067f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}