 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
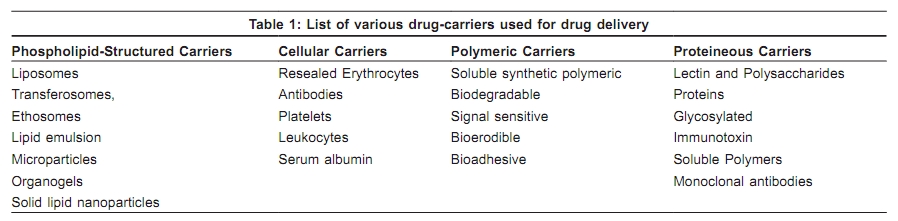
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 231-238 Review Article Topical treatment in vitiligo and the potential uses of new drug delivery systems Bhawna Jain Garg, Abir Saraswat 1 , Amit Bhatia, Om Prakash Katare University Institute of Pharmaceutical, Sciences-UGC Center of Advanced Studies, Panjab University, Chandigarh, India, Correspondence Address: Prof. O. P. Katare, University Institute of Pharmaceutical Sciences-UGC, Center of Advanced Studies, Panjab University, Chandigarh, India, drkatare@yahoo.com Code Number: dv10075 PMID: 20445292 DOI: 10.4103/0378-6323.62961 Abstract Vitiligo is a psychologically devastating condition. Topical therapy is employed as first-line treatment in localized vitiligo. Currently, several topical agents are available in many forms viz. methoxsalen (solution and cream), trioxsalen (solution), corticosteroids (gel, cream, ointment and solution) and calcineurin inhibitors (ointment and cream). Although topical therapy has an important position in vitiligo treatment, side-effects or poor efficacy affect their utility and patient compliance. Novel drug delivery strategies can play a pivotal role in improving the topical delivery of various drugs by enhancing their epidermal localization with a concomitant reduction in their side-effects and improving their effectiveness. The current review emphasizes the potential of various phospholipid based carriers viz. liposomes, transferosomes, ethosomes, lipid emulsions, solid lipid nanoparticles and organogels in optimizing and enhancing the topical delivery of anti-vitiligo agents, whilst reducing the side effects of drugs commonly used in its topical treatment.Keywords: Novel drug delivery, phospholipid-based carriers, topical therapies, vitiligo Introduction Vitiligo is an acquired idiopathic, dermatological disorder characterized by well-circumscribed milky white macules devoid of identifiable melanocytes. These asymptomatic white macules can be psychologically extremely damaging, even leading to attempted suicide in some cases. [1] It affects approximately 1% of the world's population and approximately 3-4% of the Indian population. [2],[3] The most common sites of involvement are the face (24.5%), neck (18.8%), and scalp (11.2%). [4] The exact etiology of vitiligo is unknown. It is believed that vitiligo is a polygenic trait and that a convergence theory combining elements of different etiological theories across a spectrum of expression is the most accurate etiology. [5] Treatment In general, topical monotherapy is indicated for mild-to-moderate vitiligo. Current treatment options for vitiligo include medical, surgical and adjunctive treatments. [6],[7] Medical treatment targets the immune system and helps to arrest the spread of depigmentation. In cases of stable vitiligo, repigmentation can be achieved by dermatosurgical techniques and adjunctives includes use of cosmetics. Both surgical and medical treatment have their own limitations. Adjunctive can only cover the patch and be used along with surgical or medical treatments. Medical Therapies The best studied and most commonly used medical treatment options are corticosteroids, psoralens and depigmenting agents. Corticosteroids: Topical steroids are often first-line therapy, especially in children or for localized disease. Moderately potent to potent topical corticosteroids are used. [8],[9] However, vitiligo requires prolonged use of these agents, often much longer than the usual "safe" recommended periods of use for inflammatory dermatoses. This results in significant, therapy-limiting side-effects like atrophy, hypertrichosis, peri-lesional hypopigmention etc. It is obvious that currently available dosage formulations do not provide site-specific drug delivery. Phototherapy: Phototherapy is one of the oldest forms of treatment of vitiligo and remains the bedrock of vitiligo therapy even today. Out of three [5-MOP (bergapten), 4, 5, 8-trimethylpsoralen (TMP) and 8-MOP (methoxsalen)] different types of psoralens, 8-MOP is the most commonly used. Topical psoralen photochemotherapy (PUVA) is often used for people with limited disease (affecting less than 20% of the body). It is also used for children 12 years and older, who have localized patches for vitiligo. [10] Severe sunburn, blistering and abnormally dark repigmentation are major potential side-effects of topical PUVA therapy. This is due to the uncontrolled photo- reaction of psoralen with ultra-violet A irradiation in the epidermis because drug is freely available from currently available dosage formulations, for reaction on surface after topical application. [11] In recent years, narrow-band UVB (NB-UVB, 311 nm) has become the preferred phototherapy for vitiligo. [12],[13] Calcium modulators: Recently, calcium modulators, the vitamin D3 analogues (calcipotriol and tacalcitol), have also been tried in the treatment of vitiligo. [14] Defective calcium transport has been shown in melanocytes and keratinocytes harvested from patients with vitiligo Further, vitamin D3 has been shown to activate melanin synthesis. [15] There are contradictory reports of their efficacy in vitiligo, both as monotherapy and in combination with both PUVA and NB-UVB phototherapy. The most common adverse effect of calcipotriol is lesional irritation and potential hypercalcemia if applied in quantity > 100mg in a week. So, controlled delivery can potentially deliver better results by modifying currently available dosage formulations, minimizing both systemic absorption and local irritation. Calcineurin inhibitors: Calcineurin inhibitors (tacrolimus, pimecrolimus) are some of the newest topical drugs in dermatology. [16],[17] However, tacrolimus and pimercrolimus are effective only in vitiligo lesions on the head and neck region. [18] The main difficulty with topical calcineurin inhibitors, and one that is probably responsible for lack of efficacy in non-facial vitiligo, is their high molecular weight. This precludes efficient delivery of the drug at the level of the basal cells, since the stratum corneum allows very poor absorption of any molecules over "500Da" in weight. [19] This has recently been proved by an elegant study where greatly enhanced repigmentation with pimecrolimus was achieved by using it after performing microdermabrasion on the lesional skin. [20] Hence, carrier mediated drug delivery can substantially increase their effectiveness bypassing the stratum corneum barrier and delivering these drugs in adequate concentration to the melanocytes and keratinocytes. Adjunctive Therapies Depigmentation: Depigmentation is a more drastic form of treatment, when vitiligo is extensive i.e. vitiligo universalis. Depigmentation involves fading the rest of the skin on the body to match the already white areas by using permanent melanocytotoxic agents such as Monobenzyl ether of hydroquinone cream (Benoquin; ). The major side-effect includes irritant dermatitis but rarely limits therapy. [21] A more recent method of depigmentation utilizes topical 4-methoxyphenol (4-MP) and the Q-switched ruby laser (QSR). [22] Sunscreens: People who have vitiligo are more susceptible to sunburn and long term photodamage. To prevent sun-induced darkening of the surrounding normal skin, broad spectrum high protection factor sunscreens (SPF15-30) which provide protection from both UVB and UVA light should be used. Cosmetics: Camouflage is often used to "cover" affected areas. This may be practical for patients that have minimal disease or segmental disease. [23],[24],[25] Many brands of dyes Dermacolor; (Kryolan) and Dermablend; (L'Oreal) are available in India. New Drug Delivery Systems In contrast to the traditional oral route, topical drug delivery for vitiligo has many advantages. It bypasses all major organ systems like GIT, liver, kidney etc. there by avoiding many issues of adverse effects, bioavailability etc. Nevertheless, topical application of drugs is not a simple matter. The major hurdle in producing the desired therapeutic action is the inability of the existing dosage forms like gels, lotions, creams and ointments to serve or deliver what is required, where it is required. Currently, material selection and designing of these dosage forms fails to account for the physiological and structural aspects of skin (e.g. the tough cornified stratum corneum as barrier to drug transport), while the drug related issues of high molecular weight, skin penetration, release parameters and stability are not properly addressed. [26],[27] The complex lipid and cellular structure within the cornified layer of intra-follicular epidermis, composed of ceramides, cholesterol and free fatty acids contributes to the impermeability of skin. [28] These reasons have been responsible for using systemic route for many a potential drug candidate for primary skin manifestations, whereas the topical route could have been the more appropriate choice. For example, the systemic delivery of potentially hazardous drugs like psoralen and corticosteroids through oral route has been in practice for vitiligo and many other skin diseases, as their topical products are either not very effective, or produce too many local adverse effects. [29],[30] The failure of topical conventional dosage forms is mainly accounted for by poor penetration and inability to place the drug molecules at the desired site of action for a prolonged period without allowing systemic absorption. Also the conventional dosage forms are unable to provide the protection to the normal tissues leading to "innocent bystander" side effects like dermal atrophy with corticosteroids. The drug also needs to be shielded from the local metabolic milieu of the skin, so that it is protected from breakdown into inert or toxic metabolites. Inactive metabolites would curtail drug action, requiring repeated application and toxic metabolites can produce unacceptable adverse effects. Further, in a traditional approach, the major drawback is the non-consideration of the real requirement of the drug molecule at the particular site for desired action. In this regard, a tailored system is needed to transport and target the molecule in the most effective manner. In a nut shell, all the problems associated with the conventional formulations, suggest that modifications and innovations are required in the way topical therapy is administered. Drug-carrier systems Recently, a variety of materials and methods are being used to create some very exquisitely built carrier systems. [31],[32] Some of these systems are mentioned in [Table - 1]. These carriers, with their own specificities, have attracted the formulations based on requirement and application of their field of work. The last decade has seen a phenomenal growth in the use of phospholipid-structured carriers in topical delivery. Simultaneously, it has been seen that the other carriers mentioned in [Table - 1] are also useful for oral and parenteral drug delivery. Topical drug delivery systems Phospholipid-structured carriers would be the vehicle of choice for topical delivery for vitiligo because optimized topical delivery employing these phospholipid-structured carrier systems was seen due to improved profile (pharmacokinetic and pharmacodynamic) of the chosen drug molecules for various skin diseases. [33],[34],[35] This was due to various reasons discussed below:
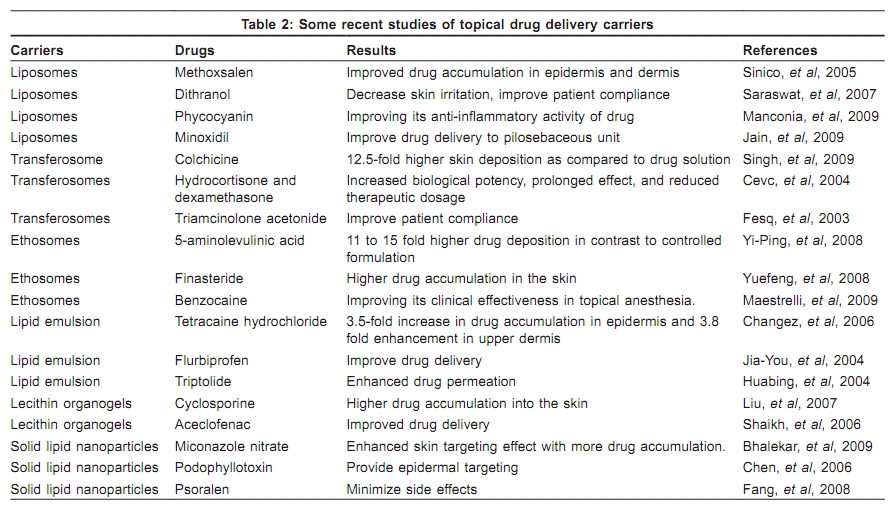
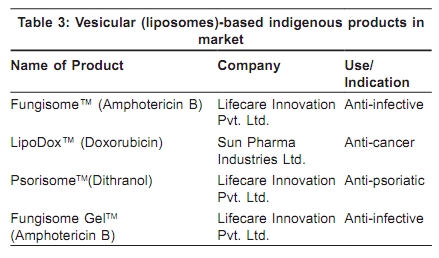
Vesicular approaches Liposomes: Liposomes are microscopic, fluid-filled pouches whose walls are made of layers of phospholipids. Liposomes were first produced in England in 1961 by Alec D. Bangham but the potential value of liposomes for topical therapy was first introduced by Mezei and Gulasekharam. Cholesterol may be included to improve bilayers characteristics of liposomes; increasing microviscosity of the bilayers, reducing permeability of the membrane to water soluble molecules, stabilizing the membrane and increasing rigidity of the vesicles. Psorisome TM , a liposomal-gel version of dithranol produced in our laboratory is one such example. Further, results of several studies [Table - 2] indicate that liposomes were useful for drug delivery in vitiligo and other dermatological disorders. [37],[38],[39],[40] Transferosomes: Cevc, et al, introduced the first generation of elastic vesicles, referred to as transferosomes. These self-optimized aggregates, with the ultraflexible membrane, are able to deliver the drug reproducibly either into or through the skin with high efficacy. [41],[42],[43] The better skin penetration ability of these elastic vesicles in comparison to liposome is supported by various studies [Table - 2]. Ethosomes: Ethosomes are lipid-based elastic vesicular systems embodying ethanol in relatively high concentrations which enhance the topical drug delivery. The presence of ethanol prolongs the physical stability of the ethosomes with respect to liposomes. The enhanced delivery of actives incorporated in the ethosomes [Table - 2] can be ascribed to the interactions between ethosomes and skin lipids. That may open the new pathways due to the malleability and fusion of ethosomes with skin lipids, which results in the penetration of drug into deeper skin layers. [44],[45],[46] Non-vesicular approaches Lipid emulsion: Lipid emulsions are thermodynamically stable, isotropic, low viscosity colloidal dispersions consisting of micro-domains of oil and/or water, stabilized by an interfacial film of alternating surfactant and cosurfactant molecules. The incorporation of lipids improves the physical stability of emulsion by forming a mono- or multi-layer around the dispersed liquid droplets which reduces the interfacial tension or increases the droplet-droplet repulsion. As topical vehicle, lipid emulsions [Table - 2] have potential to enhance the permeation and form local cargo or micro-reservoirs in the deeper skin layers to provide localized action. [47],[48],[49] Lecithin organogels (LOs): LOs are micro-structured biocompatible gels, which are chiefly comprised of phospholipids (lecithins) and appropriate organic liquids. LOs are simple in the sense that they are formed spontaneously by virtue of their thermodynamic stability. A number of therapeutic agents have been incorporated in the LOs for their facilitated transport across the skin and improve their therapeutics. [50],[51] In the wake of the commercial availability of one class of LOs, known as PLOs (Pluronic lecithin organogels) as template vehicle for topical delivery of many therapeutic agents, the importance of research in this area has increased manifold [Table - 2]. Solid lipid nanoparticles (SLNs) : They are submicron sized carriers for controlled and targeted drug delivery. Nanoparticles are diverse both in shape and composition. SLNs combine the advantages of different colloidal carriers, for instance - emulsions and liposomes. Particulate systems like nanoparticles have been used as a physical approach to alter and improve the pharmacokinetic and pharmacodynamic properties of various types of drug molecules. [52],[53],[54] Conclusion A number of drugs [Table - 3] are available in the market, which have achieved improved efficacy and safety after incorporating the active agents in carrier systems. Therefore, putting new life into erstwhile discarded drug molecules by transforming them into novel formulations can serve as viable and cost effective alternative to the expensive and time consuming search of newer chemical entities. In recent times, new excipients, refined processing techniques, and a better knowledge of the physicochemical properties of vehicles and drugs have led to the development of new delivery systems that have the potential to re-invent the topical treatments of vitiligo. The authors of this review hope that further research with enhanced collaboration between pharmaceutical and dermatology researchers will bring this hitherto untapped potential to fruition. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10075t1.jpg] [dv10075t3.jpg] [dv10075t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}