 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 239-248 Review Article Invisible dermatoses Venkataram Mysore Venkat Charmalaya Centre for Advanced Dermatology, Bangalore, India Correspondence Address: Dr. Venkataram Mysore, Venkat Charmalaya- Centre for Advanced Dermatology, 3437, 1st G cross, 7th Main, Subbanna Garden, Vijaya Nagar, Bangalore-560 040, India, mysorevenkat@hotmail.com Code Number: dv10076 PMID: 20445293 DOI: 10.4103/0378-6323.62962 Abstract 'Invisible dermatoses' is a concept which has not received wide recognition, but is nevertheless very important both clinically and histologically. The term invisible dermatoses has been used in two contexts: a) Diseases, with out definite clinical features, and are therefore "invisible" to the clinician, but yet can be diagnosed by special investigations. b) Dermatoses which present with definite and obvious clinical features, but subtle or hidden histological features and are therefore "invisible" histologically. Diagnosis of such diseases represents a great challenge to both the dermatologist and dermatopathologist. This article discusses such diseases and offers clues and tools for their diagnosis. Diagnosis of such 'Invisible dermatoses' needs proper awareness, recognition of subtle features, special stains, special investigations such as immunofluorescence and histochemistry and proper clinicopathological correlation.Keywords: Dermatoses, histopathology, invisible Introduction In a visible organ such as skin, the benefits of a trained eye being able to see what is in front of the eyes is an obvious advantage. Several well-known quotes such as: 'skin is the mirror of internal disease', 'skin is the window to internal events' reflect this unique" visibility" feature of dermatological diseases. However, many dermatoses may have such subtle or hidden features that diagnosis is difficult and special investigations and clinical correlations are needed for proper diagnosis. Thus, all dermatoses are not necessarily 'visible' and the term 'Invisible dermatoses' is applied to such dermatoses. Goethe's remark- 'what is the most difficult of all? It is to see what is in front of your eyes." applies aptly for such diseases. The phrase 'invisible dermatoses' has been used in two different contexts:
Invisible Dermatoses of the Clinician This concept was first outlined by Kligman, [1] who coined the term to define diseases which do not manifest definite clinical features, but which can be diagnosed histologically or by other special investigations- thus these diseases are invisible clinically. The diseases in this category are shown in [Table - 1]. The basic underlying principles of this concept of "clinical invisibility" are:
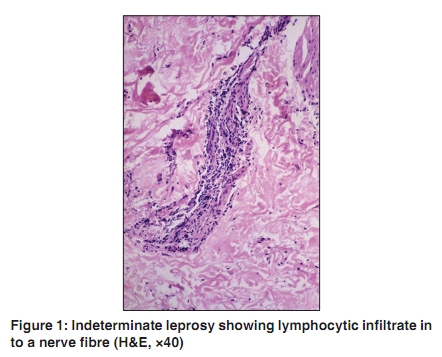
Invisible Dermatoses of the Pathologist Brownstein [3] first elucidated this concept, from the perspective of the dermatopathologist; invisible dermatoses are those skin diseases with clinically evident, and obvious skin manifestations, which however show a very subtle or hidden histological picture resembling normal skin. It is indeed paradoxical that biopsy of a clinically obvious and significant skin lesion may show an insignificant histological picture that looks apparently normal, and for this reason, these diseases have also been referred to as "Nothing diseases". Many of these conditions are not frequently biopsied as their clinical appearance is pathognomonic. Also, because the histological features are deceptively bland, the general pathologist, busy and generally disinterested in dermatopathology, is only too happy to infer that the changes are nonspecific. The diagnoses of these diseases is a challenge even to a trained dermatopathologist, and may need repeat biopsies, examination of multiple sections, special stains, special investigations such as immunofluorescence and histochemistry, and proper clinical correlatation. The list of such diseases is a large one [Table - 2]. What follows here is a brief description of some important invisible dermatoses, with clues for their diagnoses. Fungal Infections: Though the lesions of tinea corporis are not usually biopsied, cases of tinea incognito, which do not have typical clinical morphological features, may cause enough diagnostic confusion to merit a biopsy. The histological picture in tinea corporis may reveal only mild parakeratosis, spongiosis with a mild perivascular infiltrate in upper dermis. Accumulation of polymorphonuclear cells in epidermis is a helpful clue. The pathologist has to look closely for any evidence of spores or hyphae, as their number often is small. Sandwich sign [16] (presence of spores in between an upper layer of orthokeratotic stratum corneum and a lower layer of parakeratotic stratum corneum) is a helpful clue, as is the demonstration of variable refractility of spores, by moving the condenser. Periodic acid Schiff's (PAS) or silver stains for fungi can easily confirm the diagnosis. Scabies : Useful clues for diagnosis include presence of evidence of eggs, feces or adult worm. However, lesions of scabies, though characteristic clinically, may lack such pathognomonic histological features. [17] Multiple sections may need to be examined to identify the burrow. A superficial shave biopsy [18],[19] has been described as a simple, essentially painless, more reliable method for the demonstration of the scabies mite, eggs, and feces in human skin. Secondary syphilis : Secondary syphilis is becoming less prevalent in developed countries, and clinicians not familiar with this condition may resort to biopsy to elucidate the nature of rash. Secondary syphilis shows widely variable histological pictures. These include lichenoid, psoriasiform, granulomatous and rarely pseudolymphomatous patterns. [20],[21] Other common reported findings include erythema multiforme pattern of papillary oedema and perivascular lympho-histiocytic infiltration. [22],[23] Histological resemblance to indeterminate leprosy has been reported. [24] The tissue reaction is particularly mild in patients with macular lesions. The specific histological clues include plasma cell infiltrate and endarteritis obliterans, which however may not be seen in all cases. Hence silver stains may be needed for detection of Treponema pallidum. Correlation with serological tests and clinical features is essential for proper diagnosis in difficult cases. Leprosy: It is well known that in leprosy, different parts of the same lesion and different lesions in the same patient may reveal different histological pictures. Hence multiple biopsies and serial sectioning are often required for proper diagnosis. This is particularly true in indeterminate leprosy, which shows highly subtle histological changes [Figure - 1]. [25] Well-formed granulomata are absent and sections often show only mild dermal mononuclear infiltrate. A high degree of awareness and suspicion is essential to recognize the subtle histological features such as lymphocytes extending in to the arrectores muscle, perineural and periappendageal lymphocytic infiltrate. Detection of Mycobacterium leprae, which are usually scanty, needs a close search in the vicinity of nerves, sweat glands, and arrectores pilorum muscle in several sections. In a study of 56 clinically diagnosed cases of indeterminate leprosy, on routine hematoxylin and eosin (HE) and Fite-Faraco staining of paraffin embedded sections, histopathological confirmation of Indeterminate leprosy was possible in only 17 (31%) of the clinically diagnosed cases. A majority of cases were labelled as non-specific pathology. [25] Further, there is much variation between different observers. [26] It has been shown that serial sections increase the detectability of organisms and in most, if not all early lesions of indeterminate leprosy, Mycobacterium leprae would be found if an adequate number of sections stained for acid fast bacilli (AFB) were examined. Studies have shown that demonstration of mycobacterial antigen by simple and inexpensive immunoperoxidase techniques enhances the histopathologic diagnosis of indeterminate leprosy. [27] Cutaneous leishmaniasis: Lesions of cutaneous leishmaniasis usually reveal pathognomonic features of a diffuse macrophage infiltrate, with intracellular or extracellular Lesihmania-Donovan (LD) bodies, which are easily demonstrated with Giemsa stain. [28] Different histological patterns have been demonstrated in cutaneous leishmaniasis, and these depend upon the age and type of lesion, the geographic location, the strain of the Leishmania, and the immunological status of the patient: [29],[30],[31],[32]
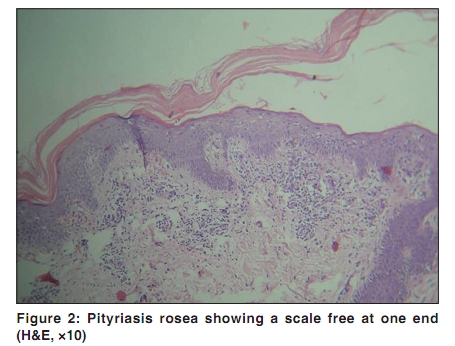
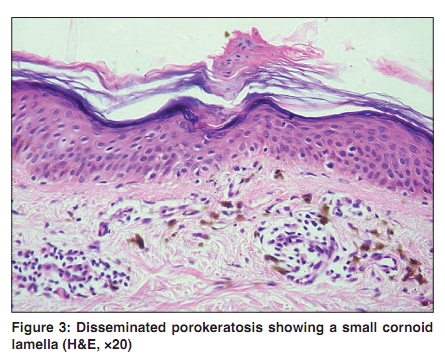
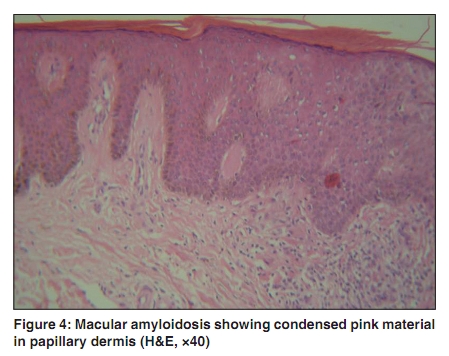
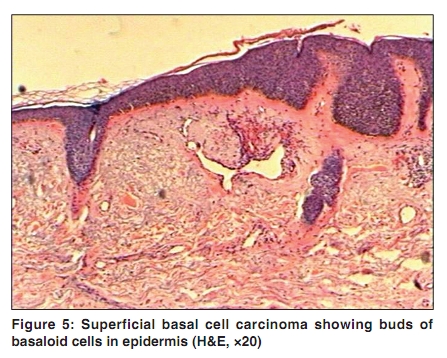
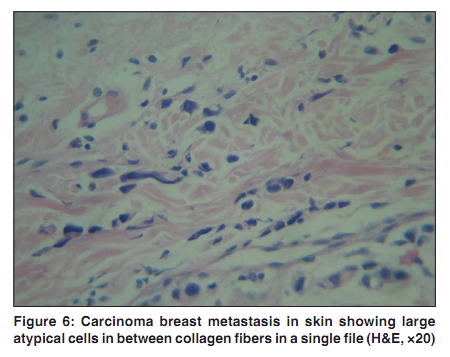
Pityriasis rosea: Pityriasis rosea is rarely biopsied as the clinical morphology is usually pathognomonic. Biopsies are performed only in doubtful cases and to rule out parapsoriasis. The histological features in this disease are usually mild and not diagnostic. [33] The main histopathological feature is the presence of a spongiotic focus in epidermis with lymphocytic exocytosis- a finding which may be seen in any dermatitis and therefore not useful for diagnosis. Other histological features include dyskeratotic keratinocytes and extravasation of red blood cells (RBCs) in the underlying dermis. Special stains are also not helpful in further elucidating the diagnosis. What is characteristic and therefore useful as a clue is the presence of this spongiotic vesicle in a clinically dry lesion. However, this spongiotic vesicle is small and needs careful search in multiple sections. Further, if the architecture of the lesion is carefully studied, a characteristic pattern, which corresponds well with the clinical architecture of the lesion, can be demonstrated [Figure - 2]. The lesion shows a peripheral zone of normal epidermis, mid zone of parakeratosis with underlying spongiosis and an inner zone of a lifting off parakeratotic scale (which corresponds to the centrifugal scale). Guttate psoriasis : Guttate psoriasis shows none of the characteristic changes of classical plaque psoriasis such as Kogoj's pustule, Munro's microabscess, and the typical regular, even elongation of rete ridges. A small parakeratotic focus with a few polymorphs may be all that is demonstrable. [34] Histological and histochemical studies of earliest changes, in two-day old lesions, revealed; (1) vascular changes, (2) inflammatory infiltrate of mononuclear cells and scanty polymorphonuclear leukocytes, (3) epidermal hyperplasia, and (4) migration of a few polymorphonuclear leukocytes through the epidermis with formation of Munro's microabscesses in parakeratotic areas of stratum corneum. [35] Another study, in very early lesions referred to as prepinpoint papules, [36] revealed fairly abundant infiltrates, composed in a large part of polymorphonuclear cells. From the morphologic viewpoint, the progression from two-day-old to fully evolved psoriatic lesions seemed basically to be quantitative. It is obvious that while these findings may offer a clue for understanding the pathophysiology of the disease, they are of limited diagnostic value. These cases need clinical correlation and proper follow up for evolution of the lesions. Granuloma annulare : In classic grauloma annulare with wellformed palisading granuloma, there is hardly any difficulty faced in diagnosis. Lymphohistiocytic granuloma with various degrees of collagen degeneration, microdroplet lipid accumulation, and mucin deposition form the basic pathologic description of granuloma annulare. [37] However in incomplete forms, changes of necrobiosis are usually mild and inconspicuous. In such cases, low power view can provide several clues; a disorganized appearance of dermal collagen, the look of a 'busy dermis' with many mononuclear cells scattered in dermis, and India filing of mononuclear cells in between collagen bundles. In the early lesions, the collagen fibers show various forms of alterations, with hyalinization and fragmentation being the most common; in half of these lesions, neutrophils and nuclear fragments in various numbers and densities have been found among the altered collagen fibers. [38] Special stains for mucin may demonstrate small amounts of mucin and thereby help in diagnosis. Porokeratosis: Cornoid lamella is the pathognomonic histological feature in porokeratosis and is typically seen in the classic Mibelli type of porokeratosis. However, in disseminated superficial type, the cornoid lamella is often small and may need careful examination of several sections before a small column of parakeratosis is revealed [Figure - 3]. Other reported helpful findings include papillary dermal lymphocytic infiltrate (97%), vacuolar changes in spinous layer (90%), dyskeratotic cells in the epidermis (77%), and liquefactive degeneration of the basal layer (67%) under the cornoid lamella. [39] Papillary lymphocytic infiltration is seen more frequently inside the porokeratotic ring in comparison to the outer skin. Lichen planus : Lichen planus is usually an easy histological diagnosis. However flat pigmented lesions may present difficulties in diagnosis. In late lesions, band like infiltrate is lost and residual features such as pigment incontinence, patchy perivascular infiltrate and basal cell vacuolation are the only features. [40] Ashy dermatoses, lichen planus pigmentosus and drug induced pigmentation all show similar histological features at this late stage. Clinical correlations are vital for diagnosis at this stage. Lupus erythematosus (LE) and other connective tissue diseases : In acute and occasionally subacute types of LE, basal cell degeneration may be the only significant histological feature. It too may be subtle and therefore be missed. Presence of edema, and vascular changes are additional, important clues. These lesions also lack the characteristic changes of discoid LE (DLE) such as follicular plugging and thickened PAS positive basement membrane. DIF for immunodeposits may help in diagnosis, but very early lesions, less than six weeks old lack significant immunodeposits and hence DIF may be false negative. [41] These cases need correlation with serological tests, and repetition of biopsy after few weeks to demonstrate evolution of lesions. Dermatomyositis shows clinically typical lesions such as Gottron's papules, which however show only mild histological changes such as basal cell vacuolation, thickened basement membrane and dermal lymphocytic infiltrate. [42] Atrophoderma of Passini and Pierini is distinguished clinically from morphoea, by the presence of a characteristic cliff border at the edge of the lesion, which is depressed and indurated. Histologically the diagnosis is difficult as the sections may not show significant changes. [43] However a comparison with surrounding normal skin will show a striking reduction in overall thickness of dermis. A biopsy from the edge of the lesion involving uninvolved skin is necessary to demonstrate this finding. Graft versus host disease (GVHD) : Diagnosis of GVHD depends on a constellation of clinical features, back ground or the setting of the patient and temporal progression of events. [44] Satellite cell necrosis-presence of a central apoptotic cell surrounded by a ring of lymphocytes- is generally considered as a suggestive change, but is often subtle in macular lesions. [45] Histological diagnosis of macular lesions in acute GVHD is usually difficult and clinicopathological correlation is important for proper diagnosis. [46] Mastocytosis: Useful clues for diagnosis in cutaneous mastocytosis include the striking monomorphous appearance of the infiltrate (due to exclusive presence of mast cells in the absence of other inflammatory cells), pronounced dermal oedema and metachromatic granules which can be demonstrated by toluidine stain. [47] A 'fried egg appearance' is considered a useful clue for recognition of mast cells. However this appearance is lacking in lymphoid and spindle type of mast cells. However, diagnosis of mastocytosis can be a challenge as it is difficult to identify mast cells in routine H and E sections, particularly if their number is small. Degranulation of mast cells due to the trauma of the biopsy itself can also lead to poor demonstration of mast cell granules. In the telangiectatic and macular types of mastocytosis, the number of mast cells is usually very small, limited to papillary dermis, spindle in shape (mimicking fibroblasts), and hence, their diagnosis is difficult. Special stains such as Giemsa stain, toluidine blue or Leder stain are essential to demonstrate the metachromatic granules. Pigmentary diseases: Several pigmentary diseases belong to the category of invisible diseases. Some diseases such as lichen planus pigmentosus, ashy dermatosis, fixed drug eruptions are discussed already above. Macular amyloidosis and argyria are two other typical examples. Macular amyloidosis: This pigmentary condition, particularly common in Asians, is characterized by pigmented macules in a characteristic rippled pattern over the arms, fore arms, and the interscapular area. The clinical diagnosis is easy. H and E stain shows mild hyperkeratosis, increased basal pigmentation, pigmentary incontinence and thick condensed collagen in papillary dermis, with mild perivascular infiltrate in upper dermis [Figure - 4]. However, demonstration of amyloid is difficult because the amount of amyloid is small. Special stains such as Congo red and thioflavine T are necessary to demonstrate amyloid. However, in many cases, even these special stains may fail to demonstrate the small amount of amyloid. Electron microscopy or immunohistochemistry is required for confirmation of diagnosis in such cases. [48] Electron microscopy demonstrates the straight fibers of amyloid just below epidermis and provides a definitive, but expensive tool for diagnosis. Argyria: Argyria on face may cause diagnostic confusion with other facial pigmentations such as melasma and lichen planus pigmentosus. While routine histology is inconclusive, detailed examination of the sweat apparatus with silver stains may demonstrate the presence of round brownish granules in argyria. [49] Similar granules are found in upper dermis in mercury poisoning. Dark ground examination can demonstrate these granules to be brilliantly refractile. Vitiligo: Clinical diagnosis of established vitiligo is always easy. However, early vitiligo lesions, may cause diagnostic confusion with postinflammatory hypopigmentation. The number of melanocytes is decreased in vitiligo, which may be difficult to demonstrate in early lesions, unless adjoining normal skin is examined. Immunostains can be helpful. While active melanocytes can be detected by DOPA and immunohistochemical staining (such as antibody NKI-beteb), amelanotic melanocytes can only be detected by the latter. [50],[51] Ultrastructural studies have shown degenerative changes in early lesions. [52] Nevus depigmentosus can also present diagnostic challenges. A study showed that, histologically, lesions of vitiligo, unlike nevus depigmentosus, showed more basal hypopigmentation and dermal inflammation than perilesional normal skin. With NKI/beteb staining, number of melanocytes was decreased in both vitiligo and nevus depigmentosus, but more in the former. [53] Cutaneous mucinoses: Diseases characterized by the deposition of mucin such as scleredema of Buschke are easily diagnosed clinically, but the mucin may be difficult to demonstrate histologically. When mucin is present in small quantities, H and E shows only mild separation of dermal collagen -a feature which can be easily overlooked. All such sections should be stained with Alcian blue or colloidal iron. [54] The biopsy specimen should be sent fresh to the lab for histochemical stains. Alcian blue stain at pH 2.5 is necessary for demonstration of acid mucopolysaccharides. Ichthyosiform diseases: Ichthyosis, whether congenital or acquired, present definite clinical features clinically and is easily diagnosed. However, histologically they show subtle features. Icthyosis vulgaris shows hypogranulosis whereas other varieties show normal granular layers. Skin in lamellar icthyosis resembles the skin of palms and soles, showing dramatic thickening of stratum corneum. [55] Neonatal icthyosiform erythroderma is another instance wherein histological opinion is frequently sought. Netherton's Syndrome (NS), can be difficult to diagnose, by routine histology, and is often misdiagnosed as atopic dermatitis. Immunohistochemistry of skin with an antibody against LEKTI is a potentially useful diagnostic test for NS. [56] Perforating dermatoses : Established lesions in any perforating disease show sufficiently diagnostic appearance and are therefore easy to diagnose. Conditions such as perforating granuloma annulare, perforating lichen nitidus etc may be missed, unless sections are properly performed to include the area of perforation. Multiple sections therefore may be needed for proper diagnosis. Early lesions of even typical perforating dermatoses may not show typical features. Early stage showed exocytosis of inflammatory cells and alteration of elastic fibers in dermis, while evidence of perforation in basement membrane was evident only in older lesions. [57] Immunohistochemistry with antibodies to the basement membrane, laminin, collagen and cytokeratin show collagen and elastin within the centre of the lesions. [58] Tumors: In several tumors, the changes may be subtle and hence invisible to the untrained eye. Large cell acanthoma, an uncommon tumour found mainly on the face of elderly individuals, is distinguished by the presence of large size of both nucleus and cytoplasm of cells in stratum Malphighi. [59] However, this appearance may not be noticed unless one observes carefully the border between the normal and the involved epidermis, where the striking and abrupt change from normal epidermis to the tumour can be appreciated. Tumors such as incipient and atrophic type of actinic keratosis, and superficial type of BCC [Figure - 5] may contain small foci of tumour cells which may need study of several sections for proper diagnosis. [60] Sclerotic/morpheic BCC may show thick bundles of collagen with thin scattered strands of basaloid cells which need close study for diagnosis. Desmoplastic syringoma is another example in which the characteristic tadpole appearance of sweat glands may be lacking as tumour masses are compressed by the thick collagen bundles. Melanoma too can be difficult to diagnose. [61] Several types of melanoma such as superficial spreading, [62] amelanotic, [63] desmoplastic [64] and minimum deviation types [65] show subtle features and therefore difficult to diagnose in early stages. Metastatic deposits may be disarmingly bland on microscopy and a close inspection is required to detect the presence of atypical cells often in an Indian file in between collagen bundles. [66] This appearance is particularly true of carcinoma breast [Figure - 6]. Immunostains with specific markers are needed for diagnosis in all such instances. Parapsoriasis and mycosis fugoides : Parapsoriasis and patch stage of mycosis fungoides are cogent examples of invisible dermatosis. While clinical lesions are characteristic in plaque and tumour stage, patch stage, particularly the hypopigmented variant presents challenges for diagnosis. Its differentiation from parapsoriasis is difficult, even for experienced dermatopathologists and previous studies have shown a low agreement rate among pathologists leading to conflicting opinions. [67] Chronic superficial dermatitis (small plaque parapsoriasis) shows banal, mild lymphocytic infiltrate in upper dermis with a parakeratotic epidermis. [68] Large plaque parapsoriasis shows a more pronounced dermal lymphocytic infiltrate, with mild epidermotropism of mononulcear cells. [69] Mycosis fungoides (patch stage) is diagnosed by the following criteria proposed by Ackerman;
Several other dermatological conditions which fall in to the category of invisible dermatoses are shown in [Table - 2]. Conclusion Invisible dermatoses present a great challenge for diagnosis clinically and histologically. Awareness of the subtle histological and clinical variations, proper clinicopathological correlation, repeated histological examination of biopsies and multiple sections, resort to advanced diagnostic techniques are important for diagnosis. Acknowledgments Sincere thanks to Dr. Anitha BS for her assistance in editing the article. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10076f3.jpg] [dv10076t1.jpg] [dv10076f6.jpg] [dv10076f5.jpg] [dv10076f1.jpg] [dv10076t2.jpg] [dv10076f4.jpg] [dv10076f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}