 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 254-258 Original Article Topical placental extract: Does it increase the efficacy of narrowband UVB therapy in vitiligo? Imran Majid Govt. Medical College and CUTIS Skin and Laser Clinic, Srinagar, Kashmir, India Correspondence Address: Dr Imran Majid, CUTIS Skin and Laser Clinic, Srinagar Kashmir- 190 010, India, imran54@yahoo.com Code Number: dv10078 PMID: 20445295 DOI: 10.4103/0378-6323.62964 Abstract Background: Narrowband UVB therapy is presently one of the most
effective therapies for generalized vitiligo. Many topical agents have
been used in combination with narrowband UVB therapy to increase its
efficacy in causing repigmentation in vitiligo. Placental extract is
used topically usually in combination with sun exposure to cause repigmentation
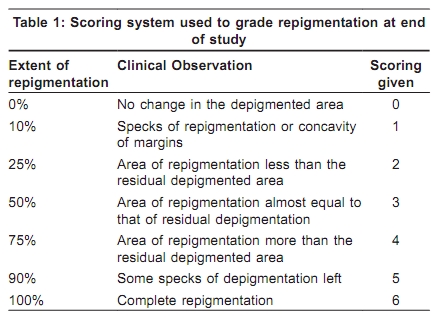
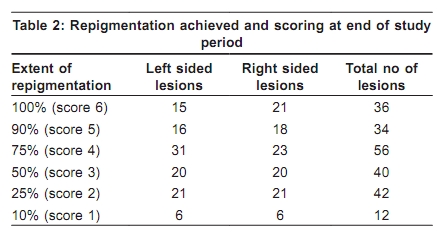
of vitiligo lesions. Keywords: Narrowband UVB therapy, topical placental extract, vitiligo Introduction Vitiligo is a very common skin disorder affecting about one to two per cent of the world population. [1] The disease is associated with profound psychological distress, especially in people with colored skin. [2],[3] The etiology of this disease is still not known with certainty and the hypothesis that is currently the most favored in the world is the autoimmune hypothesis. There are many treatment options available for this distressing disorder but none of these is universally effective. Narrowband UVB therapy has been in use for the treatment of vitiligo since the last two decades and it enjoys the status of being one of the most effective treatment options in vitiligo at present. [4],[5],[6] Many topical agents have been used in combination with narrowband UVB therapy over the years to increase the chances of repigmentation in patients with vitiligo and these include Vitamin D analogues, tacrolimus etc. [7],[8],[9],[10],[11] Human placental extract is used for the treatment of vitiligo either in the form of intramuscular injections or as a local application on the vitiligo lesions twice or thrice daily in combination with sun exposure. [12],[13],[14] How this human placental extract helps in vitiligo is not absolutely clear but it is claimed to have a mitogenic effect on the skin melanocytes as well as a stimulatory effect on the process of melanogenesis in surviving melanocytes. [15],[16] The chemical composition of human placental extract has also been studied in vitro and it has been found to contain sufficient amounts of small-molecular-weight proteins/peptides, some amino acids, glycosphingolipids, sialic acids, cholesterol, triglycerides, high density lipoproteins (HDL) and even nucleotides, carotenes and some vitamins. [17] Glycosphingolipids present in placental extract are claimed to induce adhesion, spread and motility of melanocytes. [17] Similarly endothelin, a 21-amino acid peptide present in human placenta is thought to be essential for growth of melanocytes. [17] Methods The present prospective half-and-half comparison study was conducted on 90 patients of generalized vitiligo who received narrowband UVB therapy for their disease from May 2007 to May 2008. The criteria for enrolment were presence of bilaterally symmetrical vitiligo lesions on the upper or lower limbs, face or trunk, progressive or stable disease, at least 10% body surface involvement and a high degree of motivation to adhere to the study protocol. Age less than 12 years, spontaneously repigmenting vitiligo and any known contraindication to phototherapy served as exclusion criteria. The local ethics committee at the center approved the study design prior to the start of the study. Narrowband UVB therapy was given by means of a whole body cylindrical NB-UVB chamber containing 24 high intensity NB-UVB tubes with an inbuilt dosimeter (Speigel series UVB chamber from V-care labs, Bangalore). Treatment with NB-UVB was given to the whole body three times per week on non-consecutive days according to the set protocol. The initial dose of NB-UVB was 200mj/cm 2 in all patients and it was increased at every follow-up visit by 20% of the previous dose till minimal erythema of the vitiligo lesions was achieved. Further increments, when needed were 10% of the last given dose and in case of symptomatic erythema or blistering of lesions, NB-UVB was withheld for one week and the dose was decreased by 20% of the last administered dose on resumption of NB-UVB. Lesions that were symmetrically present on the face, limbs or the trunk were selected for the comparison analysis and photographed prior to the start of the study. Lesions on hands and feet were, however, excluded from the comparison analysis owing to their known resistance to narrowband UVB therapy. Similarly vitiligo lesions less than 2cm in diameter were excluded from the comparison analysis. After enrolment into the study and after obtaining a written consent, the patients were instructed to apply topical human placental extract [placentrex lotion marketed by Albert David labs, India] on their vitiligo lesions on the right side of the body twice daily, once in the morning and then again at bed time. The patients were told to avoid any contact of the topical placental extract to the lesions on the other side which served as the control side. The patients were followed up every two weeks for the first month and once a month after that and the repigmentation of each individual vitiligo lesion was noted down at every visit by a single trained dermatologist. A simple modification of the VASI scoring (vitiligo area and scoring index) [18] was used to assess the extent of repigmentation achieved in the vitiligo lesions. Under this scoring system the extent of repigmentation of each vitiligo lesion was assessed individually as follows: 0% if there was a uniform depigmentation with no change in the overall size of the original lesion, 10% if there were just a few specks of pigmentation or just a concavity of the margins achieved, 25% if the depigmented area exceeded the area of pigmentation achieved, 50% if the pigmented area achieved equaled the residual depigmented area, 75% if the area of pigmentation achieved clearly exceeded the residual depigmentation, 90% if only a few depigmented specks were left and 100% if the whole of the original lesion got repigmented without any residual depigmentation. Repigmentation achieved was thus scored as score 0 (0% repigmentation) to Score 6 (100% repigmentation) as mentioned in [Table - 1]. Repeat photographs were taken every three months and an attempt was made to photograph lesions on both sides of the body together wherever possible. The extent (scoring) of repigmentation achieved on each side was compared at each visit and a final statistical analysis about the extent of repigmentation achieved on each side was done at the end of study period. Difference, if any between the results achieved on the two sides were tested for their statistical significance by using SPSS software for Windows and paired t-test. The duration of the study period was 12 months or till the complete resolution of vitiligo lesions if the same occurred earlier. Results Overall, 90 patients were enrolled for the present study out of which only 78 completed the study period of 12 months. Rest of the 12 patients could not continue their narrowband UVB therapy because of domestic or other personal reasons. There were no dropouts because of any adverse effects or intolerance to the treatment regimen. The age of our patients ranged from 13 to 36 years with a mean of 23.63 ±8.38 years. The male: female ratio was about 2:1 with 58 females and 32 males in the study group. The duration of vitiligo ranged from one year to 14 years with a mean of 2.4 years. All the enrolled patients had vitiligo lesions distributed symmetrically on the face, upper or lower limbs or on the trunk. Only 78 patients with a total of 218 symmetrically distributed lesions (109 on each side) were available for evaluation of results at the end of the study period and the overall results achieved are summarized in [Table - 2]. Lesions that were distributed asymmetrically on the body as well as lesions on hands and feet were excluded from the study results. On an overall basis the extent of repigmentation in the symmetrically distributed lesions (study lesions) ranged from 10 to 100% and the mean repigmentation achieved was 63%±15.7%. Complete repigmentation (score of 6 on the VASI scale) was achieved in 36 study lesions in 11 patients. Similarly, 90% repigmentation (score of 5) was achieved in further 34 lesions in 13 patients. Thus a total of 24 patients could achieve> 90% repigmentation in 70 of their symmetrically distributed vitiligo lesions at the end of study period. Another 56 lesions in 18 patients demonstrated a 75% repigmentation rate (score 4) at the end of study period while in another 40 lesions a repigmentation of 50% (score 3) was achieved [Table - 2]. Only 54 lesions in 19 patients failed to show a significant repigmentation (score 0 to 2) at the end of 12 months. Adverse effects to the treatment regimen were minor and insignificant. The commonest reported adverse effect was pruritus, seen in 11 patients. The severity and incidence of pruritus was similar on the two sides of the body and resolved of its own in all cases. Xerosis was the other side effect noted down by six patients. No phototoxic reaction was observed in any of the patients enrolled for the study. As far as the comparison of the extent of repigmentation achieved on the two contra-lateral sides was concerned we found a complete repigmentation in 21 lesions (in 11 patients) on the right side of the body (placental-extract side) compared with 15 lesions distributed symmetrically on the left side (control side). Additionally, 18 right-sided lesions achieved a 90% repigmentation rate as compared with 16 lesions on the contra-lateral side [Table - 2]. Thus on an overall basis 39 lesions achieved 90-100% repigmentation on the right (placental extract) side as compared with 31 lesions on the left or control side of the body. However, on the other hand, 43 right-sided lesions achieved a repigmentation score of 3-4 compared with 51 symmetrically distributed lesions on the left side. Lesions achieving < 50% repigmentation (score 2 or less) were distributed equally on the two sides of the body. The mean repigmentation score thus came to be 63% (VASI score of 3.69) on the right side as compared with 62% (3.60 on VASI scale) on the left side. The time and thus the NB-UVB dose needed for the onset of repigmentation was the same for lesions on the two sides of the body. Similarly the cumulative NB-UVB dosage received was the same for both the sides. Statistical analysis of the results was performed by using SPSS Windows and paired t-test and the difference in the results on the two comparison sides was found to be statistically non-significant (p value> 0.5). Discussion Narrowband UVB therapy has emerged as one of the most effective treatment options in vitiligo over the last decade. A number of clinical studies have been conducted all over the world and all of these studies have documented a positive effect of narrowband UVB therapy in vitiligo. The safety of this treatment option has also now been documented in childhood vitiligo. [6] How narrowband UVB therapy helps in vitiligo is not known with certainty but it has been postulated that NB-UVB acts at two different steps in vitiligo treatment. The first step is the stabilization of the depigmenting process and the second is the stimulation of residual follicular melanocytes. [18],[19] While the former is explained by the immunomodulatory effect of NB-UVB on the local and systemic immune responses the latter is thought to be secondary to the stimulatory effect on the dopa-negative, amelanotic melanocytes in the outer hair-root sheaths of hair follicles in the affected skin. [19],[20] Topical agents have been used in combination with narrowband UVB therapy to either increase its efficacy or minimize the total NB-UVB dosage required to cause repigmentation in vitiligo patients. Most of these topical agents have their own independent role in vitiligo and the aim of combining these agents with NB-UVB is to cause a synergistic effect on the repigmenting process in vitiligo lesions. Topical calcipotriol has been used in combination with narrowband UVB therapy in vitiligo and has shown contradictory results in two different studies reported so far in the world literature. [7],[8] While one of these studies has shown a positive effect on combining calcipotriol with narrowband UVB, the other study has failed to show any such beneficial effect of the combination. [7],[8] A right-left comparison study to evaluate the effect of topical tacalcitol with NB-UVB has shown a positive effect of the combination in comparison with NB-UVB alone in vitiligo. [9] Another agent that has shown a positive effect in combination with NB-UVB in vitiligo treatment is topical tacrolimus. [10] However, a single left-right comparison study done in a small group of 8 patients has failed to show a beneficial effect of combining topical tacrolimus with narrowband UVB. [11] Topical placental extract is used quite commonly in India in the treatment of vitiligo. The agent is used topically on the vitiligo lesions twice or thrice daily usually in combination with solar exposure to induce repigmentation in vitiligo lesions. The aim behind the current study was to see whether the efficacy of NB-UVB could be enhanced by using this topical placental extract in combination with it. And the results that we got indicate that narrowband UVB therapy lives up to its image of being one of the most effective treatments in generalized vitiligo at present. This was quite evident in our study as we were able to achieve 75% to complete repigmentation in about 66% of lesions in our study group. The adverse effects seen were also negligible and didn't require any active intervention on our part in any case. However, topical placental extract failed to show a really significant advantage when it was combined with narrowband UVB therapy. This was evident from the fact that the overall extent of repigmentation achieved was almost the same when narrowband UVB was used alone or in combination with the topical placental extract. Similarly the topical application of placental extract did not influence the mean NB-UVB dose needed to induce repigmentation in vitiligo lesions. We have been using topical placental extract in vitiligo patients and we do find it effective in some patients, especially in early vitiligo. What can possibly explain the absence of any added benefit of this topical extract in combination with NB-UVB in our study is either a predominantly chronic vitiligo that we were dealing with or the absence of UVA that may be needed to see the effect of topical placental extract in vitiligo. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10078t1.jpg] [dv10078t2.jpg] |
| |||||||||


{kind=link}
{kind=link}