 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
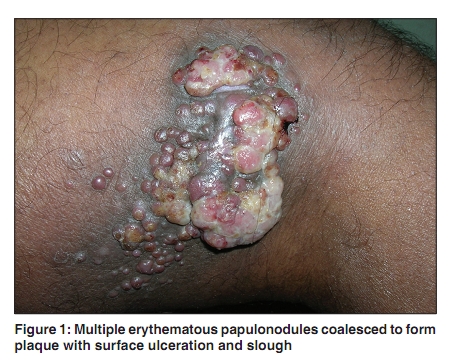
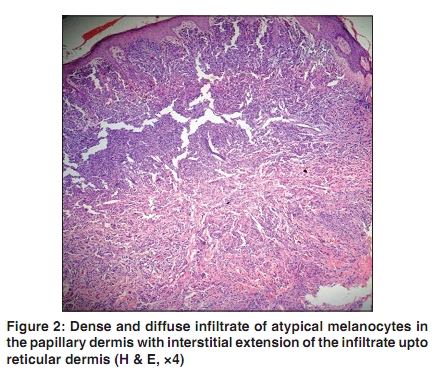
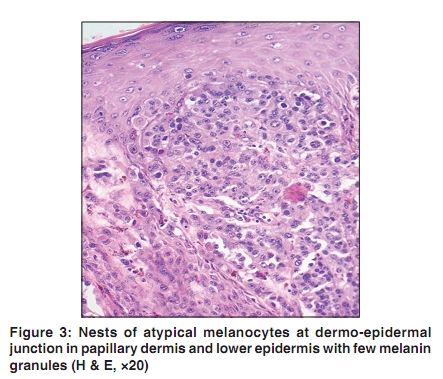
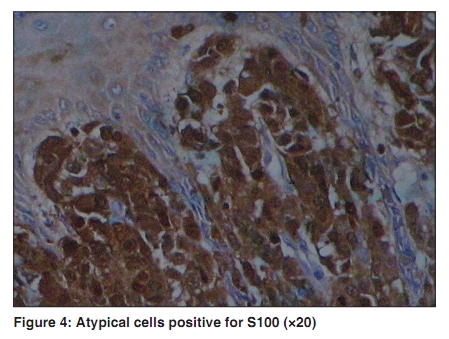
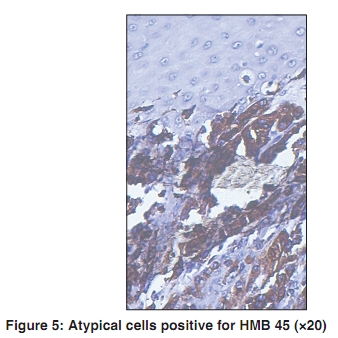
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 273-275 Case Report Nodular amelanotic melanoma Rashmi Nalamwar, Vidya Kharkar, Sunanda Mahajan, Sidhhi Chikhalkar, Uday Khopkar Department of Dermatology, Seth G S Medical College and KEM Hospital, Parel, Mumbai, India Correspondence Address: Dr. Uday Khopkar, Department of Dermatology, Seth GS Medical College and KEM Hospital, Parel, Mumbai-400 012, India, drkhopkar@gmail.com Code Number: dv10083 PMID: 20445300 DOI: 10.4103/0378-6323.62972 Abstract We report a case of 65-year-old male patient who presented with multiple erythematous papules coalescing to form a nodular mass over posterior aspect of right thigh of six months duration. His general and systemic examinations were within normal range except for right inguinal lymphadenopathy. Biopsy from the lesion was done, which showed diffuse infiltrate of nests of atypical melanocytes extending upto reticular dermis. Malignant cells were positive for S100 and human melanin black 45(HMB 45). Hence, a diagnosis of amelanotic melanoma (AM) - Clarke level IV and TNM stage III was reached. MRI of involved leg showed fungating soft tissue mass in the posterolateral aspect of right thigh and metastatic right inguinal adenopathy. Fine needle aspiration cytology (FNAC) from the right inguinal nodes confirmed metastasis of melanoma. The patient was referred to oncosurgery department for further management.Keywords: Amelanotic melanoma, HMB45, Immunohistochemistry, pigment melanin, pigmented rim or border, S100 Introduction The incidence of amelanotic melanomas (AMs) has been estimated between 1.8-8.1% of all melanomas. [1] It presents diagnostic difficulty for the clinicians, as it lacks the usual melanin pigment and no fixed criteria for diagnosis are available. The most common presentation of AMs is of nodular variety. Although AM frequently shows a few melanin granules it is often difficult to differentiate from nonepithelial malignant tumors. [2] Immunohistochemistry is an important tool in the diagnosis of AM. We report a case of AM of nodular variety. Case Report A 65-year-old male patient presented with a painless progressive nodular mass over posterior aspect of right thigh of six months duration with ulceration, slough and secondary infection at places [Figure - 1]. Initially, a few erythematous papules had appeared on posterior aspect of right thigh six months back and then several such lesions appeared and had coalesced to form a large tumor mass. There was no history of significant weight loss in the past six months nor was there history of breathlessness, upper quadrant discomfort, bony pain or any orificial bleeding. On cutaneous examination multiple, erythematous, clustered nontender papulonodules that had coalesced to form a plaque of approximate size 10Χ8 cm were present. The plaque showed surface ulceration, slough and peripheral blackish pigmentation. The involved extremity showed pitting edema and induration. Right inguinal lymph nodes were enlarged, firm, nontender and ranged in size from 2-3cm in diameter. We considered the differential diagnoses of squamous cell carcinoma, cutaneous metastasis from unknown primary, AM and lymphangiosarcoma. His routine blood biochemistry and hemogram were within normal limits. The serology for hepatitis B surface antigen, hepatitis C and human immunodeficiency virus was negative. His blood sugars both fasting (94 mg/dl) and postprandial (111 mg/dl) were within normal limits. His chest roentgenogram and electrocardiogram were within normal limits. Histopathological examination from one of the lesions showed diffuse infiltration up to reticular dermis by nests of malignant melanocytes. The cytoplasm was abundant, granular with scanty melanin granules. Mitotic figures were frequent. Clarke level was IV and Breslow's thickness was 3 mm from granular layer [Figure - 2] and [Figure - 3]. Immunohistochemistry for S100 and HMB45 was positive [Figure - 4] and [Figure - 5]. Fine needle aspiration cytology (FNAC) from right inguinal lymph node showed scattered malignant cells most of which had eccentric rounded nuclei, conspicuous nucleoli and voluminous cytoplasm compatible with metastasis from melanoma but the melanin pigment was absent. Magnetic resonance imaging (MRI scan) of the involved extremity showed soft tissue mass in the posterolateral aspect of right thigh and right inguinal adenopathy. Abdominal and pelvic ultrasound did not reveal any abnormality. The patient was referred to oncosugery department for surgical intervention where wide local excision and split thickness grafting was done. He followed up in our OPD after three months and showed no evidence of recurrence till date. Discussion The clinical diagnosis of malignant melanoma is usually based on cutaneous examination. A history of change in the color, shape or size of a previously existing pigmented lesion or de novo appearance of a pigmented lesion arouses suspicion of melanoma. In absence of usual pigmentation, it is difficult to make a diagnosis of melanoma. AM is a rare variant of melanoma which has little or no melanin pigment. Melanoma susceptibility gene is CDKN2A located on chromosome 9p21. [3] Cutaneous melanoma very often have a mutation in either NRAS or the BRAF genes, suggesting that either of these oncogenes may lead to development of melanoma due to increase signaling through the mitogen-activated protein (MAP) kinase pathway. [4] There are four clinicopathologic variants of malignant melanoma-superficial spreading, lentigo maligna, nodular and acral lentiginous. [5] AM can have any one of the above morphology but nodular is the most common variety. [5] AM may represent a primary melanoma, a recurrence of a previously pigmented melanoma, or a metastasis from pigmented primary melanoma. A peripheral pigmented rim or border can be seen in some cases which may provide a diagnostic clue. [1] Some authorities have suggested three clinical presentations for AM: an erythematous macule with epidermal changes on sun-exposed skin, a skin coloured dermal plaque without epidermal changes and a papulo-nodular lesion. [6] Histopathology and immunohistochemistry are essential for diagnosis of AM. Dermatoscopy is upcoming noninvasive diagnostic tool for AM. [7] The prognosis of cutaneous AM is determined by tumor thickness, location, and patient's age and sex - similar to its pigmented counterpart. In some cases, there is evidence of some pigment melanin on histopathology and immunohistochemistry, which includes S100 (positive for melanocytes) and HMB-45 (positive for premelanosomes). Many hypothesis have been proposed to explain the lack of pigment including: lack of tyrosinase, agenesis of melanosomes or abnormal melanogenesis, [8] while others have suggested that amelanotic tumors produce melanin, but in undetectable levels. [9] AM should be regarded as poorly differentiated form of melanotic melanoma with grave prognosis if not treated timely. [10] Acknowledgement We would like to thank Dr Nimish Mehta and Tata Memorial Hospital for helping us. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10083f1.jpg] [dv10083f3.jpg] [dv10083f5.jpg] [dv10083f2.jpg] [dv10083f4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}